The U.S. Military Use of Research & Development to Control Infectious Diseases
*Corresponding Author(s):
Ya YangGraduate Student, M.S. In Global Health Program, Curricular Design And Evaluation Assistant, Office Of Postdoctoral Development, Biomedical Graduate Education, Georgetown University, United States
Tel:+ 530-715-5168,
Email:yy578@georgetown.edu
Abstract
The U.S. military has a long history of using research and development to control infectious diseases. For more than 200 years, the military has developed vaccines and products for its troops during times of war. This paper seeks to explore how the U.S. military has controlled infectious diseases by examining the research and developments it has conducted on pharmaceutical drugs, surveillance systems, products, and capacity building. While these vaccine and products were not intended for civilians use, they became available for civilians, and the knowledge paved the path for further research studies. Overall, the civilians benefited from the research and development that the military has produced.
Keywords
Capacity training; Infectious diseases; Products; Surveillance systems; U.S. Military; Vaccines
INTRODUCTION
The U.S. military sector’s role in global public health has a long and dynamic history, and it has much involvement in health than what we know. It is rich in successes of inventions and lessons learned in failure in the prevention and control of infectious diseases. For more than 200 years since the formation of the continental army in 1770, the military has actively engaged in global public health by contributing to research and development [1]. The U.S. military’s interest in the concept of research and development was inspired by the infectious diseases that significantly contributed to the troop morbidity and mortality rates in times of war. With its troops deployed to over 160 countries around the world, including areas with endemic and infectious diseases, the military places a high priority on protecting its personnel to maintain force health and operational readiness [2]. For this purpose, it has invested in disease prevention and control efforts that have led to many scientific contributions, especially in global public health. These contributions have benefited not just only the troops but the civilians as well. This paper seeks to understand how the U.S. military has controlled infectious diseases by exploring the research and developments it has done on pharmaceutical drugs, surveillance systems, products, and capacity building.
INFECTIOUS DISEASES
Infectious diseases kill millions of people annually. Three infectious diseases were ranked in the top ten causes of death worldwide in 2016 [3]. They were respiratory infection (3.0 million deaths) which was ranked 4th, diarrheal diseases (1.4 million deaths) that was ranked 9th, and tuberculosis (1.3 million) which came as 10th. As described by the World Health Organization (WHO) [4] “Infectious diseases are caused by pathogenic microorganisms, such as bacteria, viruses, parasites or fungi; the diseases can be spread, directly or indirectly, from one person to another. It also includes zoonotic diseases, which are infectious diseases of animals that transmit to humans.” It penetrates the body’s natural barriers and creates symptoms that can range from mildly to deadly. Some infectious diseases affect the entire body while other only affect just an organ or the system of the body. Unlike non-communicable diseases, there are new infectious diseases that emerge every year. Some diseases are exactly the same, but its evolvement naturally becomes resistant to available treatments. Due to this, infectious diseases have been a persistent threat to the health of the U.S. armed forces. In fact, data from many past conflicts show that infectious diseases have caused greater morbidity and mortality than battles injuries [5]. For instance, during the end of World War I, one of every 67 U.S. soldiers died due to the influenza pandemic. Furthermore, 2 out of 3 U.S. soldiers that were admitted to the hospital during the Vietnam War were due to infections such as malaria, viral hepatitis, and diarrheal disease [5]. Until the World War II, deaths due to infectious disease outnumber those due to injuries [5]. Although many things have changed and efforts have decreased the infectious diseases at wars, the U.S. military is still consistent with focusing on research and developments efforts that are designed to mitigate the impacts of infectious diseases. These efforts have pioneered many treatments, techniques, and resources used for civilians.
U.S. MILITARY FUNDING
In 2019, the federal budget for the fiscal year was $4.407 trillion [6]. In the federal budget, there are three primary national spending categories [6]. They are mandatory spending, interest on the total national debt, and discretionary spending. The mandatory spending includes governmental programs such as Medicare, Medicaid, and Social Security [6]. The interest on the nation debt is the total debt that the U.S. government has. Lastly, the discretionary spending is the optional spending set by appropriation levels each year [6].
The discretionary programs are defense, education, transportation, veterans’ benefits and services, income security, health (discretionary only), administration of justice, international affairs, natural resources and environment, community and regional development, general science, space and technology, general government, and other [6]. Within the $1,359.00 trillion discretionary spending budget, the DoD accounted more than half, $716.00 billion, of the spending. The leftover budget is allocated for the rest of the programs. In fact, the U.S. military expenditures are more than China, Saudi Arabia, Russia, United Kingdom, India, France, and Japan combined [7]
With a lot of funding within the DoD, it demonstrates that there are a lot of resources available. The DoD allocates a chuck of resources into understanding, preventing, and treating infectious diseases that pertain to global health. The funding that congress appropriated to support DoD infectious diseases control efforts are broken in to four main component budgets – the Army, Air Force, Navy, and Defense Health Programs [2]. The funding for the Defense Health Program usually transfers to the Army and Navy. The wide resources make the U.S. military an attractive partner for disease control efforts. This resulted in many efforts that were carried out in collaboration with other U.S. agencies, including the CDC, NIH, the State Department, and USAID; non-governmental organizations; bilateral and multilateral organizations; private sector, and academic institutions [2].
U.S. MILITARY RESEARCH & DEVELOPMENT ORGANIZATIONS
In the U.S. of America, the Armed Forces are the military forces. The Armed Forces was founded on June 14th, 1775 and headquartered in The Pentagon in Arlington County, Virginia [8]. It has seven forces: Army, Marine Corps, Navy, Air Force, Space Force, Coast Guard, and National Guard [8]. The Army is the largest and oldest service in the U.S. military, and it provides the foundation forces that protect the United States. The Navy is the service that is above and under the water. According to the United States Navy, its role is “To recruit, train, equip, and organize to deliver combat ready Naval forces to win conflicts and wars while maintaining security and deterrence through sustained forward presence” [9]. Within the Navy, there is the Marine Corps. It is designed to provide on ship security and coastal invasion forces. The Air Force focuses on the flying aspect of defense. It mostly supports missions, handles base affairs, protects bases, constructs new airstrips, guard missile sites, and does rescues [10]. Moving forward, the Coast Guard provides safety and security for the U.S. maritime [11]. Finally, the Space Force, the youngest branch, was founded in 2019 to protect the U.S. and allied interests in space [12].
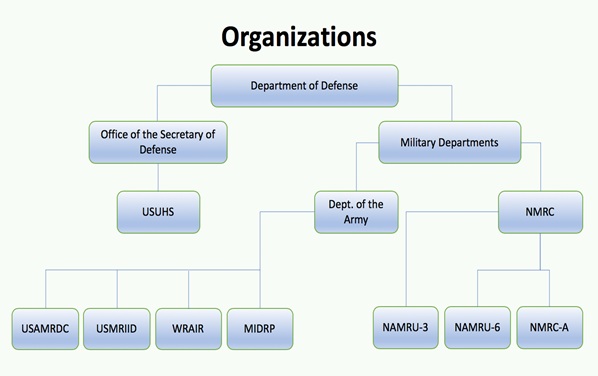
When it comes to working against infectious diseases, the DoD is categorized into two categories the Office of the Secretary of Defense and Military Departments. While disease prevents and control efforts in the U.S. military entail many sectors and organizations, the following are the primary bodies that emphasize on research and development to control infectious diseases. Organizations that involve in non-communicable diseases, leadership, or psychological research will not be discussed, because they do not pertain to infectious diseases.
|
Office of the Secretary of Defense
|
|
|
Uniformed Services University of the Health Sciences |
To reduce the impact of infectious diseases in the military population through a collaborative clinical research partnership
|
|
Military Departments
|
|
|
Department of the Army
|
|
|
U.S. Army Medical Research and Material Command |
To conduct medical research, development, acquisition, and medical logistics management for medical materiel purpose.
|
|
U.S. Army Medical Research Institute of Infectious Diseases |
To develop strategies and products for medical defense against biological warfare agents; to protect troops from outbreaks or threats to public health. |
|
Walter Reed Army Institute of Research |
To prevent, diagnose, and treat military-relevant infectious diseases such as malaria, HIV/AIDs, dengue, diarrheal diseases, multidrug-resistant organisms, and emerging diseases To protect on brain health such as behavioral health, stress, brain injury, and other psychological issues. |
|
Naval Medical Research Center |
To perform basic and applied biomedical research on infectious diseases. |
|
Naval Medical Research Unit Three |
To study, monitor, and detect emerging and re-emerging disease threats of military and public health importance. |
|
Naval Medical Research Unit Six |
To examine infectious diseases through vaccine development, strategic building, and developing surveillance systems in South America. |
|
Naval Medical Research Center Asia |
To identify infectious disease threats of the military and develop solutions to alleviate the threats in the Southeast Asia region. |
Office of the Secretary of Defense
USUHS
The Uniformed Services University of the Health Sciences (USUHS) operates under the Office of the Secretary of Defense. It is a health science university that was created by Congress in 1972 [13]. Within the academic institution, there is a program called the Infectious Disease Clinical Research Program (ICDRP). It functions though the collaboration between the Henry M. Jackson Foundation for the Advancement of Military Medicine, National Institute of Health/National Institute of Allergy and Infectious Diseases, and other military organizations. ICDRP works to reduce the impact of infectious diseases in the military population through a collaborative clinical research partnership [13]. The research conducted by ICDRP is used for military practice and to inform health policy, clinical practice, and disseminated throughout the scientific community [13]. ICDRP’s research areas include but are not limited to acute respiratory infections, deployment and travel-related infections, emerging infectious diseases and antimicrobial resistance, human immunodeficiency virus, sexually transmitted infections, skin and soft-tissue infections, and trauma-related infections [13].
Military Departments
USAMRDC
Under the Military Departments, it is where the Department of the Army is operated in. The Army is the lead of resources in the DoD program because it receives approximately $70 million of appropriated funds annually for infectious diseases research [14]. This is only less than two percent of the NIH’s average annual spending on infectious diseases and immunology research [14]. The U.S. Army Medical Research and Material Command (USAMRDC) functions within the Department of the Army. The USAMRDC is responsible for conducting medical research, development, acquisition, and medical logistics management for medical materiel purpose [14]. The basic areas that it conducts research are in military infectious diseases, combat casualty care, military operational medicine, chemical biological defense, and clinical and rehabilitative medicine [14]. The USAMRDC has contributed to research and development by developing drugs, diagnostic, and vector control products [14].
USMRIID
The U.S. Army Medical Research Institute of Infectious Diseases (USMRIID) employs under USAMRDC. The USMRIID develops strategies and products for medical defense against biological warfare agents [14]. It protects troops along with investigates disease outbreaks or threats to public health. Currently, the USAMRIID is the only DoD laboratory that is equipped to conduct research on hazardous viruses at Biosafety Level 4 [14]. It also develops medical products to protect against biological threats, such as anthrax, botulism, plague, Ebola and Marburg hemorrhagic fevers, Hantavirus, ricin toxin, and staphylococcal enterotoxin B [14]. Among the medical products, USMRIID collaborates with the Joint Biological Agent Identification and Detection System, the Centers for Disease Control and Prevention (CDC), DoD Global Emerging Infections Surveillance and Response System, and the U.S. Food and Drug Administration (FDA) [14].
WRAIR
The Walter Reed Army Institute of Research operates under the USAMRDC, and it is the largest biomedical research facility within the DoD [15]. It has developed many historical vaccines, trainings, discoveries, and programs. One of the biggest contributions to control infectious diseases was the world’s only cutaneous Leishmaniasis drug development program [15]. WRAIR hosts two centers: The Centers for Infectious Disease Research (CIDR) and the Center for Military Psychiatric and Neuroscience (CMPN) [15]. CIDR’s aims to prevent, diagnose, and treat military-relevant infectious diseases such as malaria, HIV/AIDs, dengue, diarrheal diseases, multidrug-resistant organisms, and emerging diseases. On the other hand, CMPN focuses on the protection on brain health such as behavioural health, stress, brain injury, and other psychological issues. WRAIR focuses on research and development within and outside of the United States. For example, it has established network and laboratories across four continents, including Africa, Asia, Europe, and the U.S. It also supports many stakeholders that focus in medical and biological research, including governmental institutions, pharmaceutical companies, and non-profit organizations [15].
Being the largest biomedical research facility within the DoD, the WRAIR has contributed to the development of many antibiotics, especially for malaria. For example, the WRAIR conducted clinical trials and developed Sulfadoxine-Pyrimethamine in 1983 [16]. In addition, the antimalarial drug known as Melfloquine was developed in 1989 by the WRAIR. Melfloquine is affordable and still one of the most treatments used in the military. However, side effects such as neuropsychiatric effects have been reported and malaria sites have been found to develop resistance to the drug [16]. Due to problem with the side effect, the WRAIR is currently developing antimalaria drugs that will not cause the same effects. Another product known as Halofantrine was developed by the WRAIR [16]. Similar to Melfloquine, Halofantrine has been found to cause neuropsychiatric disturbances and the development was terminated. It still has not been licensed in the U.S. One of the most recent anti-malaria drugs known as Atovaquone-Proguanil was also available due to the collaboration of the WRAIR and its partners abroad [16].
NMRC
The Naval Medical Research Center (NMRC) is an agency that operates under the military departments, and it is the Navy’s largest biomedical research facility. It performs basic and applied biomedical research. The research areas that are emphasized are infectious diseases, biodefense, military medicine, battlefield medicine, and bone marrow research [17]. NMRC’s seven subordinate commands are the Naval Health Research Center (NHRC), Naval Submarine Medical Research Laboratory (NSMRL), Naval Medical Research Unit Dayton (NAMRU-D), Naval Medical Research Unit San Antonio (NAMRU-SA), Naval Medical Research Unit Three (NAMRU-3), Naval Medical Research Unit Six (NAMRU-6), and Naval Medical Research Center Asia (NMRC-A) (Naval Medical Research Center) [17]. While all units have conducted research to control infectious diseases, NAMRU-3, NAMRU-6 and NMRC-A are the three that focus on global health [17].
NAMRU-3
NAMRU-3 was established by the U.S. Navy Bureau of Medicine and Surgery in 1946. It used to be located in Cairo, Arab Republic of Egypt but currently in Sigonella, Italy [18]. It is the oldest military medical research facility that is abroad. NAMRU receives funding through the Armed Forces Health Surveillance Center and the Department of State Biosecurity Engagement Program [18]. Its mission is to “study, monitor, and detect emerging and re-emerging disease threats of military and public health importance, as well as develop mitigation strategies against them” [19]. The unit mainly focuses on syndrome, pathogen, vector surveillance, outbreak responses, and training for health workers. As of now, researchers in NAMRU-3 are conducting basic research in a variety of areas, including drug resistance in malaria, acute febrile illnesses, Dengue fever, and several tropical and subtropical diseases [19].
NAMRU-6
NAMRU-6 was established in 1983 in Lima, Peru to examine infectious diseases [20]. Its activities involve vaccines development, strategies building, and aiding local partners to develop surveillance systems on regional infectious diseases in South America [20]. Common infectious diseases that are found in the region include malaria, dengue fever, yellow fever, Leishmaniasis, Chagas’ disease, and typhoid fever [21]. The researches that NAMRU-6 conducts are coordinated in six different departments: Department of Bacteriology, Department of Entomology, Department of Parasitology, Department of Virology and Emerging Infections, and Department of Biomedical Informatics [20]. With a broad range of research endeavors, NAMRU-6’s contribution to global health is essential in controlling infectious diseases.
NMRC-A
NMRC-A is a new initiative formed by Singaporean researchers and the Naval Medical Research Center to conduct research on infectious disease in the Southeast Asia region. It used to be known as the Naval Medical Research Unit Two (NAMRU-2) and is based in Phnom Penh, Cambodia [18]. Under the name of NAMRU-2, the unit was known as the world leader in cholera because of its development in a cholera therapeutic regimen. Furthermore, it developed the first Rubella vaccine. Currently, NMRC-A’s mission is to identify infectious disease threats of the military and develop solutions to alleviate the threats [18]. While there is a slight transition in terms activities and location, the goal of NMRC-a and NAMRU-2 is similar - to control infectious diseases.
INVENTIONS OF PHARMACEUTICAL DRUGS
Pharmaceutical drugs are often thought of being developed from the CDC, NIH, pharmaceutical companies, and researchers. However, the research and development of pharmaceutical drugs has always been a priority for the U.S. military because it protects the war fighters from endemic diseases, especially those that are infectious. Since the passing of the Kefauver-Harris Drug Amendment in 1962, there have been 28 vaccines licensed in the U.S. Out of those 28 innovative vaccines, the U.S. military played a significant role in the development of seven [22]. The inventions of vaccines have treated both troops and civilians.
INFLUENZA
There are four different types of influenza viruses: A, B, C, and. Influenza A is very diverse and found in many species. Influenza B is only found in humans, and influenza is found in mostly humans but can also be found in dogs and pigs. Influenza D is only mainly in cattle. Influenzas A and B are the two common influenzas that cause seasonal infections every year. Out of the two, Influenza A is the most complex because it can be broken down into strains. It includes the H1N1, H3N2, avian influenza, and many other subtypes.
One of the most prominent vaccine developments done by the U.S. military was the Influenza virus vaccine that became licensed in November 1945. According to the CDC [23], the number of deaths was estimated to be at least 50 million worldwide while 675,000 of the deaths occurred in the United States. During the influenza pandemic in 1918 through 1919, approximately one of out every 67 soldiers died due to the influenza [24]. Due to the large deployment of military members across the world, it may have contributed to the spread of the virus. In fact, more troops died to the influenza than from battlefield injuries. The director of the Armed Forces Epidemiological Board, Thomas Francis, collaborated with the School of Public Health from the University of Michigan, Ann Arbor and obtained the strains of the influenza and used an inactive whole-virus vaccine [24]. Furthermore, the DoD funded studies that examined the transmission and prevention of influenza, which set foundational knowledge for civilian public health officials. To date, the DoD representatives participate in the FDA Advisory Committee that analyzes influenza-related products [24].
RUBELLA
Interestingly, the U.S. military played an important role in developing vaccines for rubella, a virus that mainly affects children. While children do not participate in the military, many female hospital personnel were essential workers that treated troops. These females are typically in the age of childbearing and were at risk for rubella infection. In 1962, the rubella pandemic caused 12.5 million cases [24]. It resulted in 2,000 cases of encephalitis in the U.S., affecting 30,000 infants where there were an estimated of 6,250 unplanned abortions and 2,100 neonatal deaths [24]. To support the female workers in service, researchers from WRAIR isolated the rubella virus by using their existing virology techniques. Paul Parker from WRAIR collaborated with Dr. Harry Meyer, resulting in the isolation of the virus and creating a vaccine [22]. The vaccine demonstrated effectiveness and brought down the number of cases from 47.745 in 1969 to only 345 in 1998 [24].
ADENOVIRUS
Deploying troops abroad exposes them to crowds and areas that do not have proper hygiene, often resulting in getting the Adenovirus. Adenoviral infections include respiratory illness, eye infections, sore throat, and diarrhoea [22]. These illnesses often end up in deaths. During the World War II, 90% of the military trainees had pneumonia and was found to be associated with adenovirus [24]. Due to the number of deaths and cases from adenoviral infections, the military established a commission to conduct epidemiologic studies. In the 1950s, researchers that were non-affiliated with the military developed the formalin-inactivated type 4 and 7 vaccines and gained approval from the FDA [24]. However, the vaccine was withdrawn because of low level of effectiveness and contamination. The military jumped in and created a vaccine that is very similar to the one approved in 1950s but was scientifically known be safer [24]. The vaccine eventually gained approval and was distributed in Wyeth Laboratories [22]. The vaccine was known to be highly effectiveness in preventing adenovirus and was distributed for many civilians.
TETRAVALENT MENINGOCOCCAL VACCINE
During the Vietnam War, there was an outbreak of meningococcal disease - especially in group B and C. Annually, there was an estimated of 2,400 cases and about 170 deaths [24]. The epidemic led WRAIR to conduct studies to develop a vaccine to protect troops. Researchers conducted studies to understand the human immunologic response to meningococcus in order to successfully develop a vaccine [22]. The bacteria were more complicated than what the researchers thought and took five years to have an appropriate understanding of it [22]. The vaccine for group C was used in 1978 and has been used ever since with slight modifications as science improves [24]. The most effective vaccine today for meningococcal is the tetravalent vaccine. Even though it was developed by Connaught Laboratories Inc. in 1981 and uses its own clinical data, the entity used the same methods as WRAIR. Currently, the WRAIR is developing the group B meningococcal vaccine and hopes to disseminate findings to the public health community for prevention purposes [24]. The development of the meningococcal vaccine has not only benefited the troops, but it also benefited civilians – particularly children under the age of five years old since they have the highest incidence rate.
HEPATITIS B & A VACCINES
There are five main hepatitis viruses, and they are often referred as types A, B, C, D, and E. Type B is transmitted by sexual contact and blood-to-blood, usually leading to chronic diseases. During the Vietnam war, type B was one of the most prevalent illnesses among military members because soldiers were exposed to HBV-contaminated blood, shared needles, and sexual intercourse [24]. Hepatitis B affects more civilians than military, so the development and vaccines were not done by the U.S. military. However, the military contributed through epidemiological efforts by using their personnel as participants for studies [22]. This allowed civilian public health officials to understand the cause and methods to prevent the virus. While the U.S. military did not develop the vaccines of the Hepatitis B, they have significantly used their time to conduct research to develop a vaccine for Hepatitis A. The WRAIR cooperated with the NIH and GlaxoSmithKline to evaluate antibody responses in humans [22]. Through clinical trials, the evaluation allowed them to develop type a vaccine in 1989.
TYPHOID VACCINE
Annually, there is an estimated of 11 to 21 million cases of typhoid worldwide, where 161,000 are deaths [25]. The U.S. military’s efforts to control typhoid dates back to the Spanish-American war where one-fifth of the troops had typhoid fever and 1,500 persons died. Back in 1911, U.S. Captain Frederic Russel modified the vaccines developed by British scientists and required all the service members to be vaccinated [24]. Ever since, the U.S. military became the first entity that required all members to be vaccinated. This prevented the fever from spreading and resulted from the lowest incidence during World War I. After the first typhoid vaccine was licensed in 1914, the military continues to fund programs that aim to control the bacteria - including treatments for patients [24].
RECENT FOCUSES – COVID
Today, the COVID-19 pandemic, caused by the virus SARS-CoV-2, has remained an international health concern. As of May 15th, 2020, there were an estimated of 4,600,000 cases worldwide and a total of 300,000 deaths [26]. United States, the country with the highest rate, has approximately 1,480,000 cases and over 80,000 deaths [26]. Similar to pharmaceutical companies, researchers, NIH, and the CDC, the U.S. military is tirelessly working to develop vaccines to prevent COVID-19 from spreading. The military is gathering researchers who have worked on Ebola, Zika, and MERS for their expertise to combat this virus. As of right now, the military has developed three prototype vaccines and already begun testing on mice. They are expecting to get a vaccine ready for human trials by the end of the summer if the trials on mice go well [26].
In addition, the military is also working on developing a detection tool that will be quicker and provides a greater capability than what the U.S. currently has. An estimated of $8.4 million from the DoD have been spent on bio surveillance activities in over 30 countries to control the spread of disease [26]. There are over 61,000 personnel that are being assigned to support COVID-19 operations, and resources (ventilators, N95 masks, and test swabs) are being supplied for response effort. As of May 13, an estimated of 84,000 certified clinical COVID-19 tests were performed in the military labs and more will be performed [26]. On top of research and development, the military has been prepared by President Donald trump to disburse COVID-19 vaccines when ready. The military’s efforts to control COVID-19 are unparallel when compared to other sectors.
SURVEILLANCE SYSTEMS
According to the World Health Organization [27], public health surveillance is defined as the “continuous, systematic collection, analysis and interpretation of health-related data needed for the planning, implementation, and evaluation of public health practice.” The collection of data is important to the success of all public health initiatives, because it is updates and provides an understanding of what initiatives and resource allocations need to be changed. The U.S. accomplishments in infectious disease control could not have been done without strong surveillance systems. These surveillance systems have helped to inform the military deployments as well as gathered knowledge to civilian public health uses [28]. The military’s development in surveillance has allowed public health officials all over the world to control the spread of many outbreaks, including Ebola, Influenza H7N9, Middle Eastern Respiratory Syndrome, Corona virus and many more [29].
GLOBAL EMERGING INFECTIONS SURVEILLANCE
In 1997, the Global Emerging Infections Surveillance (GEIS) was established in response the Presidential Decision Directive (NSTC-7) which stated the U.S. was inadequate in terms of protecting its communities from emerging infectious disease threats [30]. The GEIS is tasked to maintain responsibility for infectious disease surveillance in the U.S and other nations [31]. Its focus areas are Antimicrobial resistant infections, including sexually transmitted infections, enteric infections, febrile and vector-borne infections, and respiratory infections. Many efforts that GEIS supported include West Nile Virus, avian influenza, and H1N1 [30]. In 2009, alone, GEIS partly or wholly supported projects that resulted into 112 peer-reviewed scientific manuscripts and many scholarly posters [30]. To date, there are thousands of scholarly publications and posters that have provided knowledge to civilian public health officials. GEIS’ network of laboratories is so large that it was able to conduct active surveillance in approximately in 92 countries and 500 locations [30]. It also developed an influenza strain that was selected as one of the three seed strains by the WHO [30].
ARMED FORCES HEALTH SURVEILLANCE CENTER
In 2008, as directed by the deputy of secretary of defense, the Armed Force Health Surveillance Center (FHSC) was developed to become the central epidemiological resource for DoD [29]. Upon the establishment of the new surveillance center, the GEIS became a division of the AFHSC. While the GEIS focuses on both domestic and global work, the AFHSC primarily performs infectious disease surveillance in the U.S. military [29]. The center’s mission is to enhance the health of the military-related populations by maintaining relevant and updated health surveillance information [29]. The AFHSC operates through a collaborative approach that utilizes the combined resources from the Army Medical Surveillance, the GEIS, and the Global Health Surveillance Activity [32]. The AFHSC has undertaken on a number of initiatives and projects pertaining to infectious diseases. These projects are deliberated to help both the military and civilian public health agencies to respond to international concerns that pertain to infectious diseases.
Electronic Surveillance System for the Early Notification of Community-based Epidemics (ESSENCE)
Founded in 2004 by the Walter Reed Army Institute of Research, the Electronic Surveillance System for the Early Notification of Community-based Epidemics (ESSENCE) was initially developed for early detection of bioterrorism [33]. It was later modified and expanded to use outpatient information to monitor activities that may represent a disease outbreak. ESSENCE monitors activities by scanning Military Health Systems, containing data over 9.4 million beneficiaries [33]. The software that ESSENCE uses is the same as the CDC and many of the U.S. public health departments. This allows a collaborative effort with local civilians during an outbreak [33]. As a surveillance system, ESSENCE has contributed to infectious diseases control by allowing epidemiologists and public health officers to medical situational awareness and analyzes outbreaks.
PRODUCTS DEVELOPMENT
Vector-borne diseases such as malaria, typhus, dengue, and Lyme remain a significant threat to the U.S. military. It has historically affected the U.S. military in disproportion compared to civilians because troops are often deployed in tropical and subtropical areas. Vector-borne diseases transmit by a variety of insects, such as mosquitoes, ticks, san flies, and biting midges [34]. Annually, it accounts for more than 17% of all infectious diseases on average, contributing to 700,000 deaths [35]. Because it is a major concern among troops, the U.S. military has contributed significantly by developing projects to control the vector-borne diseases from spreading. Products that the U.S. military developed include insecticides and diagnostic products. Because vector-borne diseases remain a threat to the military, products are continuously being developed to prevent future outbreaks.
INSECTICIDES
As defined by the International Union of Pure and Applied Chemistry [36], insecticides are “pesticide used for the control of insects.” Insecticides are used by both civilians and the military, but mainly in the military because of its deployment in tropical areas that contain high rates of insects. From 1942 to 1945, the War Department within the DoD supported the U.S. Department of Agriculture (USDA) and developed over 20,000 insecticides and repellents [34]. Dimethyl phthalate (DMP) and Indalone were tested and shown to be very effective as protection against berry bugs [34]. In addition, a very prestigious lotion known as DEET was discovered. DEET was used to combat the spread of Leishmaniasis among troops, and its effectiveness against insects lasted for 12 hours [37]. After years of using DEET, research showed that troops found it to be effective but painful. In response to this concern, the U.S Army and the USDA collaborated to develop a different formulation that lasted longer and was less painful. The formulation was named as Extended Duration Topical Insect and Arthropod Repellent (EDTIAR), and it conveys six-14 hours of protection [34]. To date, EDITIAR is used by the U.S. and other militaries all over the world. Despite the decrease in wars, the military’s effort to develop finer insecticide products is still a continuous process.
DIAGNOSTIC PRODUCTS
Diagnostic products are devices that diagnose human infections that come from vector-borne diseases. During World War II, there were 5, 4441 cases and 283 deaths from scrub typhus [38]. To control the spread of scrub typhus, the U.S. military contributed to the development of the Scrub typhus diagnostic kit by funding Dr. Helen Paxton’s of Integrated Diagnostics through its Small Business Innovative Research Program (SBIR). In addition, the Malaria (Vector) Dipstick Assays, that was used to detect Plasmodium circumsporozoite protein in the mosquito vector, was also developed through the SBIR [38]. Even though the assay is no longer available due to very few purchases, the military is constantly working to bring this product back for unexpected future use. Furthermore, the SBIR supported the West Nile virus dipstick [39]. This assay is utilized to detect West Nile virus infection in insect vectors. It is very simple and rapid to use, taking only 15 minutes to get the results [39].
CAPACITY BUILDING TRAINING
Infectious diseases often impact low-and-middle income countries, but it does not mean that it will not affect high-income countries. Because of its ability to spread, it is important that all countries are prepared to contain infectious diseases. In addition to the products that were developed to detect and treat infectious diseases, the U.S. military also developed capacity building training for both the U.S. and other countries. WRAIR, for example, is known for sharing their disease control techniques to other nations. It has trained thousands of health officials in the U.S. and over 1,000 globally, including countries like Azerbaijan, Georgia, Armenia, and Ukraine. Most of the trainings include strengthening health infrastructures, disease surveillance, and outbreak investigation [40].
Furthermore, the U.S. military is known for training scientists to respond to emergency situations, both from a humanitarian and research perspectives. For example, during the Swine Flu Pandemic in 2009, the Naval Medical Research trained 73 scientists from 32 countries on the molecular diagnosis of the flu [41]. The training was shown to be effective and essential because it happened within 3 weeks of the declaration of the pandemic. This indicated that it was done in a timely manner. Overall, the capacity building trainings developed by the military has helped with the alleviation of infectious diseases.
CONCLUSION
The U.S. military has significantly contributed to the control in infectious disease through research and development. Its substantial resources allowed adequate centers to be established to conduct research and develop products. While this research and developments were intended to be done to benefit the troops, the inventions do not solely benefit the DoD. As a matter of fact, it had pioneered many medical solutions, such as vaccines, surveillance system, products, and trainings. As the military continues to establish its portfolio of activities to control infectious diseases, its contributions should not be overlooked. With the resources from the DoD, different health sectors should seek to expand future collaborations to control infectious diseases.
AUTHOR CONTRIBUTIONS
Ya Yang conducted the literature review and wrote the manuscript. The charts were also developed by Ya Yang.
REFERENCES
- Brooks RB. (2017) Continental soldiers in the revolutionary war
- Moss K, Michaud J. (2013) The U.S. Department of Defense and global health: Infectious disease efforts. The Henry J. Kaiser Family Foundation.
- The top 10 causes of death. (2018) World Health Organization.
- Infectious diseases. (2020) World Health Organization.
- Strategy for Minimizing the Impact of Naturally Occurring Infectious Diseases of Military Importance Committee, et al. Protecting Our Forces: Improving Vaccine Acquisition and Availability in the U. S. Military, edited by Stanley M Lemon, et al. National Academies Press, (2002) ProQuest Ebook Central.
- Breaking down the US federal budget. (2020) Up to Us.
- S. military spending vs. the world. (2015) National Priorities Project.
- Our Forces. (2020) United States Department of Defense.
- Who we are. (2020) America’s Navy.
- Air force mission. (2020) United States Air Force.
- United States coast guard historian’s topics. (2020) United States Coast Guard.
- S. space force fact sheet. (2020) United States Space Force.
- Infectious Disease Clinical Research Program. (2019) IDCRP.
- Military Infectious Disease Research Program (MIDRP). (2020) United States Army Medical Research and Development Command.
- Walter Reed Army Institute of Research. (2020) History.
- Military Infectious Disease Research Program (n.d.). History and achievements.
- Chiarella, Donald. (2005) History of Naval Medicine.
- NMRC subordinate commands .Naval Medical Research Center (n.d.).
- Wagner DJ. (2019) NAMRU-3 Moves to Sigonella, Italy. U.S. Naval Forces Europe-Africa/U.S. 6th Fleet.
- A look inside: Navy medicine’s Peruvian research lab, U.S. Naval Medical Research Unit no.6 [photos]. Navy Medicine Live. (n.d.).
- Naval Medical Research Unit No.6, Lima, Peru .Naval Medical Research Center (n.d.).
- Kitchen LW, Vaughn DW. (2007) Role of the U.S. military research programs in the development of U.S.-licensed vaccines for naturally occurring infectious diseases. Vaccine 25:7017-7030.
- 1918 Pandemic. (2020) Centers for Diseases Control and Prevention.
- Artenstein AW, Opal JM, Opal SM, Tramont EC, Peter G, et al.( 2005) History of U.S. military contributions to the study of vaccines against infectious diseases. Mil Med 170: 3-11.
- (2020)World Health Organization.
- Coronavirus: DoD response. (2020) United States Department of Defense.
- Public health surveillance. (2020) World Health Organization
- Pages F, Faulde M, Orlandi-Pradines E, Parola P. (2010) The past and present threat of vector-borne diseases in deployed troops. Clinical Microbiology and Infection 16: 209-224.
- Global emerging infections surveillance. (2020) Military Health System.
- Russell KL, Rubenstein J, Burke RL, Vest KG, Johns MC, et al. (2011) BMC Public Health 11:S2.
- Global Emerging Infections Surveillance and Response System. (2020) Military Health System.
- DeFraites RF. (2011) The Armed Forces Health Surveillance Center: Enhancing the Military Health System’s public health capabilities. BMC public health 11:S1.
- Electronic surveillance system for the early notification of community-based epidemics. (2020) Military Health System.
- Kitchen LW, Lawrence KL, Coleman RE. (2009) The role of the United States military in the development of vector control products, including insect repellents, insecticides, and bet nets. Journal of Vector Ecology 34: 50-61.
- Vector-borne diseases. (2020) World Health Organization.
- Stephenson GR, Ferris IG, Holland PT, Nordberg M, et al. (2006) Glossary of terms relating to pesticides. Pure Appl. Chem 78: 2075-2154.
- Crum NF, Aronson NE, Lederman ER, Rusnak JM, Cross JH. (2005) History of U.S. military contributions to the study of parasitic diseases. Mil Med 170: 17-29.
- Scrub typhus diagnostic kit. (2020) Military Infectious Diseases Research Program.
- West Nile virus dipstick. (2020) Military Infectious Diseases Research Program.
- Department of Health Services.
- Blazes D, Russell K. (2011) Joining forces: civilians and the military must cooperate on global disease control. Nature 477: 395.
Citation: Yang Ya (2020) The U.S. Military Use of Research & Development to Control Infectious Diseases. J Infect Non Infect Dis 5: 030.
Copyright: © 2020 Ya Yang, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.