Case Report: An Unusual Presentation of Syphilis in a HIV Positive Patient-“Don’t Forget the Bones”
*Corresponding Author(s):
Carole KhawAdelaide Sexual Health Centre Formally Clinic, 275, Infectious Diseases Unit, Royal Adelaide Hospital, Adelaide, SA, Australia
Tel:+61 408822025,
Email:carole.khaw@sa.gov.au; carole.khaw@adelaide.edu.au
BACKGROUND
Syphilis has been classically referred to as the “great imitator” of diseases with versatile symptomatology and presentation [1]. Syphilis rates have increased in recent years particularly in men and in majority of cases, men who have sex with men (MSM).Co-infection with HIV may result in atypical manifestations and curious presentations of early acquired syphilis.
CASE REPORT
The patient is a 56-year-old HIV positive MSM. His HIV was diagnosed in 2001 and at time of presentation, suppressed on combination antiretroviral therapy (lamivudine, raltegravir, darunavir and ritonavir). He had had good CD4 counts of over 500 cells/mm3, the latest at presentation, being 590 cells/mm3.
His General Practitioner (GP) referred him to an Ear, Nose and Throat (ENT) Physician because of a 2-month history of pain in tonsillar area and dysphagia. This wasassociated with feeling unwell, frontal headaches and fever. The ENT physician noted unusual ulcerated lesions with a white exudate on the patient’s tonsillar surface (unfortunately, no images were available) and was concerned regarding the possibility of a lymphoma.
A contrast CT scan of the head and neck was performed showing prominent adenoidal tissue noted at the posterior pharynx. The pharynx and larynx were otherwise normal. A large number of prominent cervical lymph nodes were seen although none were reported to be pathologically enlarged. No brain masses or any acute intracranial pathology were seen.
The ENT physician also considered biopsy of the adenoidal tissue to exclude lymphoma but this was not done.The patient also developed pain in his shins and extensor surfaces of his forearms. This had occurred over 6 weeks, about 2 weeks after commencement of his tonsillar pain and dysphagia. He also complained of discomfort in his elbows, wrists and ankles, affecting his sleep.
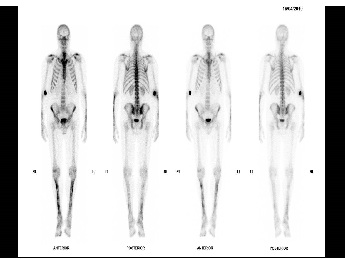
X-rays were performed of upper and lower limbs and these were unremarkable. Bone scans were then performed and these revealed patchy linear periosteal uptakes in the both tibia of legs, both ulnar and radius of forearms (Figures 1 and 2) suggesting radiological evidence of a periostitis.
The radiologist then reported syphilis as a possible cause of the radiological findings.

The patient’s GP eventually performed syphilis serology.
The results showed that syphilis screen -Enzyme Immuno Assay (EIA) was reactive, Rapid Plasma Reagin (RPR) was 1:256 and TreponemaPallidum Particle Agglutination (TPPA) Test was reactive.
His syphilis serology 6 months prior to the onset of his symptoms and signs were negative.
The patient was referred to Adelaide Sexual Health Center for review and treated with a stat dose of 1.8 mg of benzathine penicillin Intramuscular injection (IMI).
He developed a Jarisch- Herxheimer reaction within 12 hours of his penicillin injection.
On review 2 weeks following treatment with penicillin, his tonsillar lesions and shin/forearm tenderness had mostly resolved. Further follow up eventually showed a greater than four-fold drop of his RPR to 1:16 at 6 months post treatment.
DISCUSSION
Bone and joint pain are recognized findings in congenital syphilis (saber shins) BUT are far less common findings in acquired disease [2].Bone involvement often occurs in long bones and also in the skull [2]Patients in acquired disease present with pain over bony regions.
The plain radiographs are often negative. Bone scintigraphy shows increased uptake in areas of disease involvement [2].
Syphilis and syphilitic bone disease should be considered in HIV positive patients at risk of other STIs (some MSM) presenting with orthopaedic complaints or bone lesions.
Case studies have suggested that treatment should be extended for bone involvement but there have been no extended studies validating these [1,3-6].Our patient responded to 1 dose of 1.8g benzathine penicillin with improvement and eventual resolution of bone pain and on follow up, his RPR titers had dropped adequately. There was no need for extension of treatment. The patient’s initial tonsillar lesions may have been chancres of primary syphilis or mucosal lesions of secondary syphilis. Unfortunately, no syphilis PCR was performed on the tonsillar lesions. The lesions completely resolved after 1 dose of benzathine penicillin.
KEY POINTS
- Bone disease can represent an atypical manifestation of early acquired syphilis.
- HIV positive patients who present with orthopaedic complaints or bone lesions should be evaluated for syphilitic bone disease.
- Be on the lookout for periostitis in patients with syphilis who present with extremity pain.
- Isotope bone scans (Technetium - 99m bone scintigraphy) are useful in clarifying the clinical picture and defining the extent of involvement as well as picking up early lesions.
CONSENT
The patient consented to this case being reported.
REFERENCES
- Fabricius T, Winther C, Ewertsen C, Kemp M, Nielsen S (2013) Osteitis in the dens of axis caused by Treponemapallidum. BMC Infect Dis 13:347.
- GurlandI, Korn L, Edelman L, Walach F (2001) An Unusual Manifestation of Acquired Syphilis. Clin Infect Dis 32:667-669.
- French P (2007) Syphilis. BMJ 334: 143-147.
- Chapel TA (1980) The Signs and Symptoms of Secondary Syphilis. Sex Trans Dis 7: 161-164.
- Pleimes M,Hartschuh W, Kutzner H, Enk AH, Hartmann M (2009) Malignant Syphilis with Ocular Involvement and Organism-Depleted Lesions. Clin Infect Dis 48: 83-85.
- Zetola N, Engleman J, Jensen T, Klausner J (2007) Syphilis in the United States: An Update for Clinicians With an Emphasis on HIV Coinfection. Mayo ClinProc82: 1091-1102.
Citation: Khaw C and Ratnayake M (2019) Case Report: An unusual presentation of Syphilis in a HIV positive patient-“Don’t forget the bones”. J AIDS Clin Res Sex Transm Dis 6: 026.
Copyright: © 2019 Carole Khaw, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.