Epithelioid Choroidal Melanoma in a Middle-Aged Filipino: A Case Report
*Corresponding Author(s):
Jo Michael M ManiwanOphthalmology Resident, Rizal Medical Center, Philippines
Email:maniwanjo@gmail.com
Abstract
Background: To present a case of choroidal melanoma in a 49-year-old male patient.
Case Presentation: A 49-year-old male presented with an eight-month history of gradual blurring of vision of the left eye accompanied by eye pain, left-sided headache, eye redness, gradual proptosis and opacification of the cornea. Ocular ultrasound revealed a homogenous echodensities with moderate echogenicity and intermittent loculation occupying the whole vitreous cavity. Chest CT-scan with contrast showed multiple nodules on both lung fields evident of metastasis. The patient was lost to follow and sought consult 1 year after presenting with a 5x4.8cm grapelike mass with discharge and occasional bleeding, resistance on retropulsion. Incision biopsy was done and revealed epithelioid pigmented melanocytes with enlarged pleomorphic nuclei and prominent nucleoli.
Keywords
Choroid; Malignancy; Melanoma
Background
Ocular Melanomas are the second most common type of melanoma after cutaneous. It arises from melanocytes situated in conjunctival membrane and uveal tract of the eye [1]. Uveal melanomas encompass the iris, ciliary body and the choroid. In the Philippines, uveal melanoma is the second most common intraocular malignant tumor which accounts for 8% of all intraocular malignancies [2]. Choroidal melanomas are more frequent to occur in comparison to iris and ciliary body melanomas [3,4]. We present a case of choroidal melanoma in a 49-year-old Filipino who presented with an eight months history of gradual blurring of vision, eye pain and progressive proptosis with evidence of metastasis.
Case Presentation
A 49-year-old male visited the Rizal Medical Center outpatient department with a chief complaint of proptosis of the left eye. He had an eight-month history of gradual blurring of vision of the left eye accompanied by eye pain, and left-sided headache which prompted consult with assessment of cataract. During the interim, there was loss of vision, eye redness and gradual proptosis of the left eye. These ocular symptoms were accompanied by weight loss and occasional body malaise. He had unremarkable past medical, past ocular, family and personal history. Ocular examination of the left eye showed no light perception, and a visual acuity of 20/20 on the right eye. On gross examination, there was gross proptosis on the left eye with resistance on retropulsion and absence of bruits with severe chemosis (Figure 1). Anterior segment examination showed an opacified cornea with diffuse uptake, shallow anterior chamber with no view of the lens. Examination of the right eye was unremarkable. 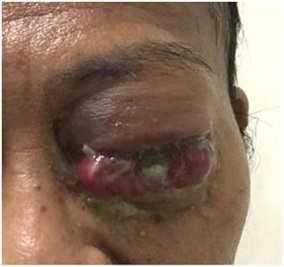
Figure 1: Clinical photograph of the left eye with gross proptosis, chemosis and opacification of cornea.
A B-scan ultrasound of the left eye revealed homogenous echodensities with moderate echogenicity and intermittent loculation occupying the whole vitreous cavity (Figure 2) with an impression of an intraocular mass with a plan to do enucleation of the left eye.
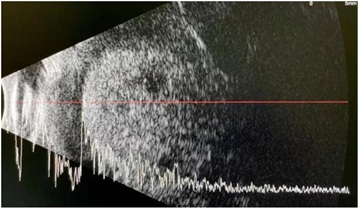 Figure 2: B-scan ultrasound of the left eye with homogenous echodensities with moderate echogenicity and intermittent loculation occupying the whole vitreous cavity.
Figure 2: B-scan ultrasound of the left eye with homogenous echodensities with moderate echogenicity and intermittent loculation occupying the whole vitreous cavity.
Chest CT-scan with contrast revealed multiple subcentimeter pulmonary nodules in both lungs with a consideration of a metastatic process (Figure 3). Abdominal CT-scan with contrast, however, did not reveal nodules, masses or lymphadenopathy. The patient was referred to oncology for metastatic work-up and palliative care but he was lost to follow-up and noted significant increase in proptosis and outgrowth of the intraocular mass which prompted consult after one year. Gross examination of the left eye revealed a 5×4.8cm grapelike mass with discharge and occasional bleeding, resistance on retropulsion (Figure 4). Visual acuity of the right eye was 20/20 with unremarkable ocular examination of the anterior and posterior segment. Incision biopsy was performed getting 3 tissues from the mass, adjacent conjunctivae and skin.
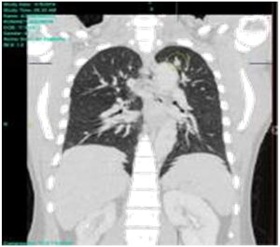 Figure 3: Chest CT-scan with multiple non-enhancing subcentimeter nodules seen in the right upper and middle lobe, and in the apical segment of the left upper lobe (encircled in yellow).
Figure 3: Chest CT-scan with multiple non-enhancing subcentimeter nodules seen in the right upper and middle lobe, and in the apical segment of the left upper lobe (encircled in yellow).
 Figure 4: Clinical photograph of the left eye (1 year after) with a 5×4.8cm hyperpigmented grapelike mass with discharge and bleeding.
Figure 4: Clinical photograph of the left eye (1 year after) with a 5×4.8cm hyperpigmented grapelike mass with discharge and bleeding.
The pathologic examination using hematoxylin-eosin stain showed epithelioid pigment melanocytes with enlarged pleomorphic nuclei and prominent nucleoli (Figure 5A) and necrotic debris with degenerated cells with cytoplasmic melanin (Figure 5B). Adjacent conjunctivae revealed evidence of chronic conjunctivitis (Figure 6A) while the skin was otherwise normal (Figure 6B). The patient was referred back to oncology for management and palliative care.
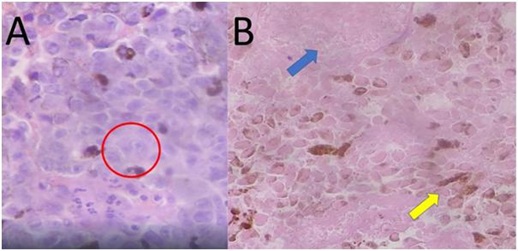 Figure 5: High power objective (original magnification x 40) of ocular mass tissue. A) Epithelioid pigmented melanocytes with enlarged pleomorphic nuclei and prominent nucleoli (encircled in red); B) Necrotic debris (blue arrow) and degenerated cells with cytoplasmic melanin (yellow arrow).
Figure 5: High power objective (original magnification x 40) of ocular mass tissue. A) Epithelioid pigmented melanocytes with enlarged pleomorphic nuclei and prominent nucleoli (encircled in red); B) Necrotic debris (blue arrow) and degenerated cells with cytoplasmic melanin (yellow arrow).
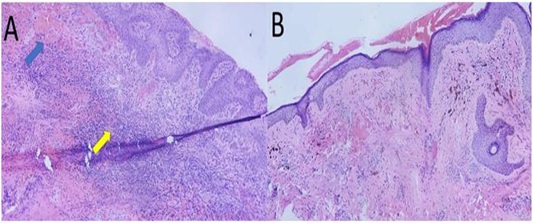
Figure 6: Low power objective (original magnification x 10) of A) adjacent conjunctivae with Conjunctival hemorrhage and thrombosis (blue arrow) and subepithelial inflammation (yellow arrow); and, B) adjacent skin with normal epidermis and subcutaneous tissue.
Discussion
Uveal melanomas are highly malignant epithelial cancers [5] which tend to commonly arise during the 5th to 6th decade wherein 65% of patient is over the age of 50 years. Risk factors include: light eye color, fair skin, Caucasians of Northern European descent, UV radiation exposure, xeroderma pigmentosum, and oculodermal melanocytosis [4]. Patients remain asymptomatic until the tumour has grown sufficiently to become necrotic and produce complications such as endophthalmitis, massive intraocular hemorrhage, and/or secondary glaucoma. Choroidal melanoma usually presents with blurring of vision, painless and progressive visual field loss as the peripheral melanoma enlarges, floaters, and flashes of light in cases of necrosis of tumor or hemorrhage in the adjoining areas [3]. The choroid being devoid of lymphatics hence majority of the choroidal melanomas spread by hematogenous route mainly to the liver and lungs [6].
The modified Callendar’s classification of uveal melanoma has five categories: 1) Spindle A cell type tumors comprise 5% of all choroidal melanomas, 2) Spindle B & fascicular comprise 39%, 3) Pure epithelioid cell melanomas comprise 3%, 4) Mixed cell melanoma (combination of spindle and epithelioid types) comprise 45% and 5) Necrotic cell type comprise 7% [7]. Among the five types, the epithelioid cell type has the lowest survival rate at 28%.
Conclusion
Pure epithelioid cell choroidal melanoma is the rarest among the cell types and has the worst prognoses which correspond to the histopathologic findings of our patient. Early detection is ideal but would pose a challenge due to its asymptomatic presentation during the early course of the disease and symptoms that mimics other ocular diseases. Complete ophthalmologic examination and high degree of suspicion combined with ocular and systemic imaging would help patients with this pathology. In the current scenario, treatment is preferably palliative and tailored toward the patient’s symptomatology.
References
- Jovanovic P, Mihajlovic M, Djordjevic-Jocic J, Vlajkovic S, Cekic S, et al. (2013) Ocular melanoma: An overview of the current Int J Clin Exp Pathol 6: 1230-1244.
- Domingo RED, Manganip LE, Castro RM (2015) Tumors of the eye and ocular adnexa at the Philippine Eye Research Institute: a 10-year review. Clin Ophthalmol 9: 1239-1247.
- Shukla S, Acharya S, Dulani M (2015) Choroid Melanoma - A Rare Case Report. J Clin Diagn Res 9: ED09-ED10.
- Krantz BA, Dave N, Komatsubara KM, Marr BP, Carvajal RD (2017) Uveal melanoma: epidemiology, etiology, and treatment of primary disease. Clin Ophthalmol 11: 279-289.
- Font RL, Spaulding AG, Zimmerman LE (1968) Diffuse malignant melanoma of the uveal tract. A clinicopathologic report of 54 cases. Trans Am Acad Ophthalmol Otolaryngol 72: 877-895.
- Kath R, Hayungs J, Bornfeld N, Sauerwein W, Hoffken K, et al. (1993) Prognosis and treatment of disseminated uveal melanoma. Cancer 72: 2219-2223.
- McLean IW, Zimmerman LE, Evans RM (1996) Reappraisal of Callender’s spindle A type of malignant melanoma of choroid and ciliary body. Am J Ophthalmol 86: 557-564.
Citation: Maniwan JMM, Valera E, Martin A (2021) Epithelioid Choroidal Melanoma in a Middle-Aged Filipino: A Case Report. J Ophthalmic Clin Res 8: 079.
Copyright: © 2021 Jo Michael M Maniwan, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.