Evaluation of the use of a manual to support a large-scale implementation of the “Estratégia amamenta e alimenta Brazil”
*Corresponding Author(s):
Glaubia Rocha Barbosa RelvasSecretaria De Estado De Saude De Mato Grosso, Cuiaba, MT, Brazil
Abstract
Objective: To evaluate the implementation of the Tutor Support Manual of Estratégia Amamenta e Alimenta Brasil (EAAB) – the "Manual", developed to support Continuing Education Activities (CEA) in primary health care.
Methods: Evaluative research with a quantitative and qualitative approach. The evaluated intervention consisted of the use of the Manual by the tutors of Embu das Artes-SP. The Manual proposes the development of five CEA with the health team. The data collection, before and after the intervention, comprised: 1) knowledge test for tutors and health workers; 2) questionnaire with the managers of the basic health units (UBS) on the implementation of the intervention and compliance with the EAAB certification criteria proposed by the Ministry of Health. A listening workshop was held with key informants on the use of the Manual. A quantitative analysis of the implementation indicators and a qualitative analysis of the listening workshop were used.
Results: The Manual was used by eight out of 13 tutors. The median of CEA performed at the UBSs was 5 [0-5]. The mean number of correct answers of the tutors (pre 31.43 ± 5.25; post 34.86 ± 4.45; p=0.021) and workers (pre 26.09 ± 4.45; post 30.28 ± 3.55; p=0.002) in the final knowledge test was higher than in the initial test. The number of certification criteria reached by UBSs was higher in the post-intervention period (median: pre 3 [1-6]; post 5 [3-6]) and was consistent with the perception of changes by managers, as well as with the number of CEA conducted by tutors.
Conclusions: The use of the Manual improved the knowledge of tutors and health workers and promoted positive changes in the work process of the teams.
Introduction
Breast Feeding (BF) and adequate Complementary Feeding (CF) in the first years of life offer, in the short and long term, benefits for the health and development of the baby, in addition to economic and environmental advantages for children, women and society in high-, middle- and low-income countries [1,2].
Since 2013, Estratégia Amamenta e Alimenta Brasil (EAAB) has been adopted by the Brazilian Ministry of Health for the promotion of breastfeeding and healthy CF in Primary Health Care (PHC). EAAB is based on the critical-reflexive methodology, proposed by Paulo Freire. Applied to the work process, it enables, through criticism and reflection, the exchange and transformation of knowledge, valuing in the group not only scientific knowledge, but also other types of knowledge, such as historical, social, cultural, economic, and experiential knowledge [3].
The objectives of EAAB are to qualify the assistance provided by the health teams and to improve child feeding practices in the Brazilian population. The basic health unit (UBS) can be certified at EAAB if it meets six criteria required by the Ministry of Health: 1 - Develop systematic actions to promote breastfeeding and healthy complementary feeding; 2 - Monitor the indicators of breastfeeding and CF; 3 - Have an instrument for organizing child health care related to breastfeeding and complementary feeding; 4 - Comply with the Brazilian Norm for Commercialization of Food for Infants and Young Children, Nipples, Pacifiers and Baby Bottles; 5 - Have at least 85% of the primary care team participate in the workshops developed; 6 - Comply with at least one action to encourage breastfeeding and one for healthy complementary feeding agreed in the action plan prepared by the PHC teams [4]. When a UBS meets all the criteria, the manager may apply for certification from the Ministry of Health.
The implementation of EAAB involves the person of a tutor, a health professional who goes through a training workshop to perform the function of support to the health teams, in the context of continuing education, for the development or strengthening of actions aimed at promoting breastfeeding and healthy CF. At UBSs, the implementation of EAAB begins with a first six-hour workshop, conducted by the tutor with the entire team, which aims to raise awareness of the workers to the issue in question and begin the development of an action plan for the promotion of breastfeeding and CF. This plan should include the realization of complementary activities from the perspective of continuing education that will be facilitated by the tutor. The Continuing Education Activities (CEA) should be oriented to the achievement of the certification criteria in EAAB [4].
However, data presented by the Ministry of Health reveal important challenges for the implementation of EAAB on a large scale, since they show that the number of certified UBSs is still insignificant and that the number of tutors trained is almost three times greater than the number of supervised UBSs. This scenario shows the obstacles faced in the performance of tutors, who should conduct CEA with the PHC teams and support the UBS certification.
Studies that evaluated the implementation and impact of the breastfeeding promotion strategy prior to EAAB and that adopted a similar methodology showed similar weaknesses in the performance of the tutor [5,6]. Thus, understanding the tutor as a key element for the success of the implementation of EAAB and facing the need to guide their actions, the authors of this study, in close cooperation with the Ministry of Health, prepared the Tutor Support Manual of Estratégia Amamenta e Alimenta Brasil (the Manual), which clarifies to the tutor what its role is and suggests themes, content and methods for the development of CEA as follow-up after the First Workshop at the UBS. The Manual follows a critical-reflexive methodology, seeking to propose an educational process applied to the work, with the objective of promoting changes in relationships and processes.
The hypothesis of this study is that the availability of a support material that defines guidelines for the performance of the tutor may facilitate and qualify their performance, contributing to improve the performance of health workers and to strengthen the implementation of EAAB. The intervention evaluated in this study was the use of the Manual by the tutors, which was designed to support them in continuing education activities, during the process of implementing the EAAB. Thus, the objective of this study was to evaluate the implementation of the EAAB Tutor Support Manual, seeking to identify the means by which this intervention can improve infant feeding practices.
Methods
Characterization of the study and context
An evaluative research of the implementation analysis type [7], with a quantitative and qualitative approach, was carried out to analyze the use of the EAAB Tutor Support Manual in the context of the implementation of this strategy in the UBS of Embu das Artes-SP, Brazil. The area of evaluation of interventions has developed a lot, and the evaluative research that is dedicated to evaluate not only the results or net effects of the programs (impacts), but also the intervening mechanisms associated with these effects has been valued. Evaluating the implementation of a program is particularly important when the intervention analyzed is complex and composed of sequential elements in which the context can interact in different ways. The implementation analysis consists precisely in specifying the set of factors that influence the results obtained after the introduction of an intervention [7].
The case study strategy was chosen because it is a phenomenon that cannot be isolated or dissociated from its context [8]. The municipality was the unit of analysis.
The city of Embu das Artes is part of the metropolitan region of São Paulo, with a population of 240, 230 inhabitants, and has 15 UBSs and 30% coverage of Estratégia Saúde da Família [9]. At the beginning of this study, the municipality had 13 UBSs and 13 tutors trained in a workshop held by the State Department of Health of São Paulo but had not started the process of implementing EAAB.
Study stages
Together with the managers of the UBS of Embu das Artes, information was collected on BF and CF actions developed, and a knowledge test was applied to tutors and health workers. After data collection, the Manual (the intervention) was made available to the tutors, and after eight months, a second data collection was conducted. These collected data allowed the quantitative evaluation of the categories of analysis and indicators built based on the conceptual model of the intervention. A qualitative evaluation was conducted based on the report of a listening workshop with the tutors, commissioned by the Ministry of Health during the period of use of the Manual. Figure 1 shows the steps of the research, which will be detailed below.
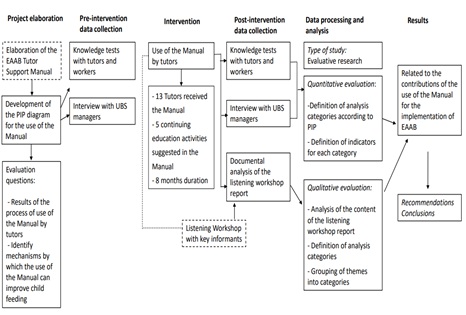 Figure 1: EAAB Estratégia Amamenta e Alimenta Brasil; PIP Program Impact Pathway; UBS Basic Health Unit.
Figure 1: EAAB Estratégia Amamenta e Alimenta Brasil; PIP Program Impact Pathway; UBS Basic Health Unit.
The intervention
The EAAB Tutor Support Manual was previously prepared by the authors of this study, according to the needs presented by the technical team of the Ministry of Health.
The intervention evaluated here consisted of the use of the Manual by the tutors of Embu das Artes for a period of eight months (November 2015 to July 2016), in the context of implementation of EAAB. The 13 tutors received the Manual and were guided by the research coordination to use it according to its suggestions. In order to support the tutor and contribute to the achievement of the EAAB certification criteria by the UBS, the Manual proposes five CEA that address the following themes: I - Action plan: agreement and definition of a work plan; II - Work process; III - Clinical management of breastfeeding in Primary Care; IV - Healthy complementary feeding in Primary Care; V - Food and Nutritional Surveillance. Each CEA has a maximum duration of 2h30min.
Conceptual model of intervention impact mechanisms (Program Impact Pathway analysis)
Traditionally, the evaluation of the implementation of interventions has been based on logical or conceptual models. While these types of program representations facilitate strategic planning and management, and provide an overview of the program, most of them do not spell out the mechanisms by which activities actually occur and achieve their impact. Some authors propose that understanding the logic of the program and how programs can achieve their effects (the impact pathways) is necessary to inform decision making and scale-up processes [10,11].
Thus, we chose to use a conceptual model of the intervention based on the Program Impact Pathways (PIP) approach, which was proposed to evaluate the implementation of programs in order to explain the stages of mediation between the inputs and results of the program following a causal logic [12]. The analysis through PIP provides a visual tool for tracking how the intervention stages have been implemented, and how the activities are expected to be linked to have an impact on immediate, intermediate and final outcomes, focusing on the different pathways of activities and influences along the way. In addition to the logical sequence of inputs, outputs and outcomes, conceptualizing impact pathways is a useful approach to understanding the causal connections required for impact and to identifying where attention and effort may be needed in the operationalization of the program [10].
In this study, the PIP diagram was prepared, first, to identify the ways and mechanisms by which the use of the EAAB Tutor Support Manual can contribute to the improvement of child feeding practices, considering the context of implementation of EAAB; and second, it was developed to define indicators of the process of using the Manual.
The logical sequence of the PIP diagram included five dimensions (1) inputs; (2) activities; (3) outputs; (4) outcomes; and (5) impact [13]. The development of the intervention PIP was conducted based on the review of the EAAB implementation documents, the activities proposed in the Manual, as well as a literature review on evaluation methodologies and program implementation. The PIP was initially developed by the first author (GRBR), and then discussed and improved with input from the other co-authors.
Data Collection And Analysis
Quantitative data
The data collection aimed at obtaining information on the implementation of the intervention from the different agents involved: managers of the 13 Basic Health Units, 13 EAAB tutors in the municipality and 153 health workers who participated in the CEA performed by the tutors. Considering that the Ministry of Health does not make any specific recommendation on the percentage of workers from the teams who should participate in the CEA developed by the tutors, the intervention was performed among the UBS workers directly involved in the implementation of EAAB indicated by the managers.
Pre-intervention data collection occurred between August and September 2015. The intervention occurred between November 2015 and July 2016. Post-intervention data collection occurred between August and September 2016. The following data collection instruments were used, depending on the subject: 1) tutors and PHC workers: self-applied knowledge test in relation to the BF and CF content, with 45 questions, based on an instrument with similar purpose proposed by Toma [14]. The application of the tests to the tutors was conducted by the researcher; the health workers answered the tests at the time of the first CEA (pre-test) and the last CEA (post-test) performed by the tutor; 2) managers of the UBS: self-administered semi-structured questionnaire.
The analysis plan was based on the PIP diagram shown in Figure 2. From the dimensions of PIP, it was possible to determine five categories of analysis: 1. Use of the Manual; 2. Activities performed with the teams; 3. Change in the knowledge of the tutor; 4. Change in the knowledge of workers; 5. Change in the work process. Then, indicators were built from the empirical data collected, based on one or more sources of information – questionnaire with managers and knowledge test applied to tutors and workers, as already detailed in the data collection. The data were entered in the EpiInfo program and those statistically treated were analyzed in the Stata 12.0 program. A descriptive analysis of the variables was performed by absolute frequency or proportion measurements, and for the quantitative variables, the central tendency measures were calculated. As the data did not present a normal distribution, the mean of correct answers before and after was compared using the non-parametric tests: Wilcoxon rank-sum (Mann- Whitney) test for the total sample (independent samples) and Wilcoxon signed- rank test in the comparison of the pairs that answered the initial and final tests (repeated samples).
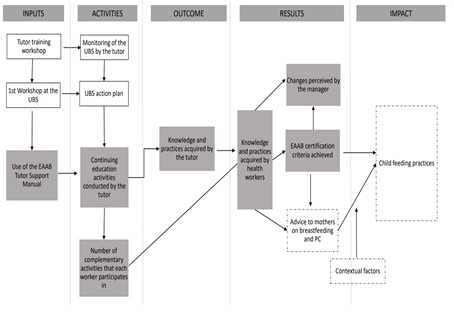 Figure 2: Solid filling: data obtained and analyzed; solid outline: EAAB implementation stages (not analyzed); dotted outline: data not obtained in this study.
Figure 2: Solid filling: data obtained and analyzed; solid outline: EAAB implementation stages (not analyzed); dotted outline: data not obtained in this study.
The PIP diagram components represented with a dotted line were not analyzed in this study, either because they represent the broader context of EAAB implementation or because they are the subject of another publication.
Qualitative data
The qualitative approach was chosen in order to complement the quantitative data in order to provide more elements for the interpretation of the results in the process of evaluating the use of the Manual. To obtain the data, we used the documental analysis technique based on the report of a listening workshop with key informants commissioned by the Ministry of Health and conducted by an external institution not involved in the process of using or evaluating the Manual. The researchers were authorized to use this report. The Ministry of Health considered as key informants the eight EAAB tutors who were using the Manual in the municipality of Embu das Artes, and all of them participated in the workshop, which aimed to listen about the process of using the Tutor Manual.
The content analysis methodology [15] was used to seek an approximation of the perception of the tutors about the potentialities and challenges regarding the content and applicability of the Manual. The workshop report with key informants was the corpus of the research and the recording units were phrases that represent a synthesis of the statements of the tutors and some of the statements transcribed in the report. We proceeded to an initial and intensive reading of the document to apprehend the record units, classifying them by core meaning (semantic criterion) which originated the themes. The themes that emerged were grouped into three previously established categories of analysis: Potentialities of the EAAB Tutor Support Manual; Suggestions for improving the Manual; and Challenges for applying the Manual.
Ethical issues
The project was approved by the Research Ethics Committee of the School of Public Health of the University of São Paulo, under protocol number 43317315.0.0000.5421, and the questionnaires, tests and interviews were applied after signing the Free and Informed Consent Form.
Results
Conceptual model
The PIP for the use of the Manual was represented in a diagram (Figure 2) that seeks to explain the paths and expected results of the implementation of this intervention, considering the context of implementation of EAAB.
The "Inputs" dimension integrated the necessary components to start the use of the Manual by the tutor, such as the Tutor Training Workshop and the First Workshop at the UBS. In the "Activities" are found both the stages of implementation of EAAB itself, as well as those inherent to the application of the Manual. "Product" refers to the immediate result expected from the use of the Manual, i.e., changes in the knowledge and practices of tutors. "Results" consisted of the intended changes in the knowledge and in the work process of the teams. Thus, based on the performance of the tutor (from the perspective of continuing education), the aim is to promote changes, first in the knowledge and practices of the workers that will reflect in the counseling practices with the mothers; and secondly in the teamwork process, in this case, expressed by the number of certification criteria achieved by the UBS. Also, in this dimension, the perception of the UBS managers about the intended changes was considered as an important aspect. The "Impact" dimension expressed the expected effect of the use of the Manual on the target population, i.e., on the infant feeding practices; in this dimension the existence of contextual factors that interfere in the skills and practices of mothers/caregivers and, finally, in the feeding of children, was considered.
Quantitative analysis
The analysis results of the implementation of the use of the EAAB Tutor Manual guided by the intervention PIP are presented in Chart 1.
|
Dimension |
Analysis Category |
Indicators |
Results |
|
Inputs |
1. Use of the Manual |
Number of tutors who used the Manual. |
8 out of 13. |
|
Activities |
2. CEA carried out with the teams |
Median of CEA conducted in the UBS (n=13). |
The median was 5 [0-5] CEA performed in the UBS. Seven UBSs performed 5; one UBS performed 4; three UBSs performed 2 activities; and two UBSs did not perform CEA. |
|
Median of activities that workers participated in (n=31). |
Among the 31 workers who answered this question, the median of participation was 5 [1-5] CEA. |
||
|
Outputs |
3. Change in the knowledge of the tutor |
Median and mean (±standard deviation) of correct answers in the pre (n=13) and post (n=7) tests. |
Median: pre-30 [21-42] versus post 34 [29-43] points. Mean: 30.77 (± 6.13) versus 34.86 (± 4.45) points, p=0.087. Considering only the 7 tutors who answered the initial and final tests: only 1 had the same score, the others improved in the post-test (mean 31.43 ± 5.25 versus 34.86 ± 4.45; p = 0.021). |
|
Outcomes |
4. Change in knowledge of workers |
Median and mean (±standard deviation) of correct answers in the pre (n=62) versus post (n=46) intervention knowledge test. |
Median: pre-27 [16-39] versus post-30 [16-37] points. Mean: 26.68 (± 4.85) versus 30.11 (± 4.26) points, p=0.000. Considering only the 22 workers who answered the initial and final tests: 17 improved the performance in the test, 1 had equal performance and 4 had a worse performance (mean 26.09 ± 4.45 versus 30.28 ± 3.55; p= 0.002). |
|
5. Change in the work process |
1. No. of pre and post intervention certification criteria (n = 13 UBSs). |
After the intervention the number of certification criteria met by 10 of the 13 UBS increased, 2 UBS remained with the same number and 1 UBS decreased the number of criteria met. Median: pre-3 [16] versus post-5 [3-6] certification criteria met. |
|
|
2. No. of certification criteria achieved after intervention, according to perception of managers in relation to change in practices (n = 13 UBSs). |
All managers perceived a change in practice after the intervention, 4 referred to it as "many changes" and 7 as "some changes". Two did not respond. Of the 11 managers who reported changes, 7 were from UBSs who met 5 or 6 criteria and 4 from UBSs with 3 or 4 criteria. |
||
|
3. No. of certification criteria achieved after the intervention according to the number of CEA carried out (n = 13 UBSs). |
Of the 8 UBSs that carried out 4 or 5 CEA, all met 4 to 6 certification criteria. |
Chart 1: Analysis matrix of the implementation of the use of the EAAB Tutor Support Manual: quantitative approach.
EAAB – Estratégia Amamenta e Alimenta Brasil; UBS – basic health unit; CEA - continuing education activities
The EAAB Tutor Support Manual was used by eight of the 13 tutors who received the Manual. The reasons why five tutors did not remain in the study were: retirement, dismissal and risk pregnancy. The eight tutors performed CEA according to the Manual in 11 UBS; one tutor performed these activities in four UBSs. The five CEA proposed in the Manual were conducted in seven of the 13 UBSs. In four UBSs, the number of activities was lower than the five recommended, and in two UBSs, there were no activities based on the Manual. The total number of health team workers involved in the CEA was 153 (mean of 13.9 per UBS), but the number of activities in which each worker participated varied. Of the 86 workers (56.2%) who answered the knowledge tests (pre- and/or post-intervention), 31 informed how many/which CEA they participated; among these, 21 answered having participated in the five activities.
Regarding the category "Change in the knowledge of the tutor", data were obtained from 13 tutors in the pre-test, but seven in the post-test. In the comparison by pairs, the average increase in the scores of the seven tutors who answered the initial and final tests was 3.4 points; p = 0.021. In the general comparison, there was a higher mean of correct answers in the post-test, without statistical significance. Among the tutors, nine were nurses, one physician, one nutritionist, one speech therapist and one dentist.
Regarding the knowledge of health workers, data from 62 pre-tests and 46 post-tests were recorded, with a significantly higher mean of correct answers in the post-test. The profile of the workers was: 62% community health workers; 27% nursing technicians; 7% nurses and 1% of each category: physician, speech therapist, psychologist and dentist. Of these, only 22 workers answered the initial and final tests, and there was also an increase in the average post-test score in the comparison of the pairs: mean increase of 4.2 points; p = 0.002. The increase was greater in the score of the workers than that of the tutors.
The indicator of change in the work process was the achievement of the EAAB certification criteria by UBSs. There was an increase in the number of certification criteria met by UBSs after the intervention: 13 managed to engage 85% of the team workers in the workshops and complied with NBCAL; 11 performed BF and CF systematic actions and had a child health care organization tool. The criteria that constituted barriers to certification were compliance with the action plan and monitoring of the indicators, met by seven and eight UBSs, respectively. The relationship between the number of certification criteria achieved and the perception of changes by managers was consistent. The perception of change was more frequent in UBSs that achieved a greater number of criteria. There was also consistency in the relationship between the number of criteria achieved and the number of CEA performed: the number of certification criteria achieved was higher in UBSs that developed more CEA, indicating a dose-response effect of the intervention in changing the work process of health workers.
Qualitative analysis
The results of the implementation analysis of the use of the EAAB Tutor Support Manual based on the report of the workshop with key informants are presented in Chart 2, showing the themes that have emerged in the three analysis categories. 1) The category "Potentialities of the EAAB Tutor Support Manual" includes reports that describe the Manual as an instrument that guides the actions, causes reflections, besides offering knowledge update and expansion. The application of the approach of the Manual to other themes besides BF and CF was also pointed out as a potentiality of the material. 2) Suggestions for improving the Manual were mainly related to the sequence and duration of some CEA and the reorganization of the annexes and appendices. 3) As for the challenges for the application of the Manual, issues related to management, continuing education, team adherence to activities and work process emerged. In the reports about the challenges, the difficulties for applicability and incorporation of the Manual stand out, among which can be pointed out the lack of management support, overload and dynamics of working with the team, time available to ensure the performance of the activities and the continuity of the continuing education process.
|
Categories |
Themes |
|
|
Potentialities of the EAAB Tutor Support Manual |
|
Content and presentation of the Manual Objective, clear, guiding, practical Offers updated content Easy language. It is a manual with an active methodology. Identifies sources and references. Provides a sequence of continuing education activities. Flexible. Allows changing the order of the activities, according to the need and demands of the Unit. Contributions to the performance of the tutor The tool is an excellent facilitator, effective and guides actions. It triggers reflections It expands and brings new knowledge. It is a manual to clarify doubts. Offers a case study with a problem situation. Provides security to carry out the activities and to adapt them to different realities. Provides pedagogical support. Provides continuity to the work and references. Provides work guidance and organization. Applying the approach of the Manual to other themes Participation of the unit manager in the activities enables the understanding that the content and methodology of the Manual can be implemented for other topics, such as the care line. |
|
Suggestions for improving the Manual |
Present more clearly at the beginning of the Manual the conditions required for UBS certification. Review the structure of the Manual in relation to the order of inclusion of annexes and appendices to improve readability and linearity. Need to review the duration of one continuing education activity (time and size). Review of the sequence of content in some activities. In some continuing education activities, the time allocated to "Closing" the activity is insufficient. Include other themes/activities to continue the work. Have the Manual in electronic format. Have a communication channel - "contact us" - for questions. |
|
|
Challenges for the application of the Manual
|
Management Lack of awareness and management support. Lack of support and participation of the Unit manager. If the managers participated in the workshop, they could offer support and create conditions for the tutor to play their part. Continuing education Ensure the continuity of the work. Guarantee the execution of the actions that were proposed and maintain the meeting with the purpose of continuing education. Adhesion of the team to the activities Team discouragement. Remove workers from their jobs and bring the team together for activities. Train the entire team of the Unit. Participation of the workers (interdisciplinarity). Work process Work overload by the tutor. Many cumulative tasks. Lack of time to attend the meetings with the municipal coordination. Lack of time for implementation, supervision and completion of activities. Allow more time to prepare for the activity, time to read the Manual and study more. Lack of human resources at the UBS. Monitoring of the educational groups carried out by the nursing team. Schedule the date (reconcile the schedule of workers) and ensure the performance of the activity. Difficulties related to personal skills Difficulty in appropriating the contents of the Manual. The fear of forgetting the script of each activity motivated the creation of reading/registration/summary forms. |
|
Chart 2: Matrix for the analysis of the implementation of the use of the EAAB Tutor Support Manual: qualitative approach based on the report of the workshop with key informants.
EAAB – Estratégia Amamenta e Alimenta Brasil
Discussion
This study innovates by proposing a support material to the EAAB tutor and evaluating its implementation process. The EAAB Tutor Support Manual proved to be a useful tool in the continuing education process at PHC, as it improved the knowledge of tutors and workers and promoted changes in the work process of the teams. Thus, this study offers a real contribution to the challenge of the Ministry of Health to advance in the effective implementation of EAAB and achievement of its objectives, to improve the skills and abilities of PHC workers and improve the actions for the promotion of breastfeeding and healthy CF.
The partial adherence of tutors to the intervention, as well as the low participation of workers in CEA, reflect the perceptions that emerged in the listening workshop with tutors about the lack of support from the manager. The insufficient participation of the tutor in the process of implementation of new technologies in PHC was previously identified in a study on the degree of implementation of Rede Amamenta Brasil, a strategy prior to EAAB with similar implementation process [5]. The analysis of the challenges for the incorporation of the Manual into the practice/routine of the UBS revealed issues of great relevance to municipal management, related to the work overload of the tutor, the team work process and the lack of support from the UBS manager. Such challenges are among the main limiting factors for the effectiveness of continuing education in health within the meta-synthesis of the literature, which also draws attention to the scarce debate around the integral health care by managers and administrators, under pressure from the demand for services, pedagogical and resource limitations [16].
On the other hand, in the analysis of the degree of use of the Manual, it is necessary to consider those tutors who effectively used the material, who presented in their reports the perception that the Manual guided the action, induced the reflection and increased knowledge. The positive change in the knowledge of the tutor observed here to a certain degree is in line with a study that, by employing active teaching-learning methodologies, favored the development of skills by nursing students involved in the education and promotion of child health, enabling them an effective and coherent approach with the role of future health workers [17]. Our hypothesis is that this result can be attributed to the use of the Manual, which offers specific content on BF and CF in the "Questions and Answers" sections, and to the possible use of the recommended complementary bibliography in the preparation of each CEA, which was reinforced by the workshop reports. Likewise, it was observed a higher level of knowledge in breastfeeding and CF by the workers after the intervention, reinforcing the hypothesis that the well oriented and active tutor in his/her functions favors the process of continuing education of the workers.
However, the small sample of workers who responded to the tests was a limitation of this analysis. If, on the one hand, the effect of the intervention may have been overestimated if these are the most interested and applied workers, on the other hand, it is likely that the small number and the few categories of workers involved in the CEA underestimated the effects of the intervention, i.e. the effects of using the Manual would have been greater if it had reached a larger number of workers. The average success rate in knowledge tests higher among tutors than among workers can be explained by the difference in the level of training, since tutors have higher education (a prerequisite for being eligible as a tutor), and among workers only 11% are university-level workers (data not presented). On the other hand, the greater increase in post-intervention knowledge in the score of workers in relation to tutors indicates that the educational intervention may have produced a greater benefit for those with lower level of knowledge, suggesting that investing in greater participation of workers in CEA is a sensitive mechanism for achieving the objectives of EAAB [4].
An important issue to be discussed in this analysis is the limitation of the "true/false" type of knowledge tests by assessing only the dimension of knowledge, i.e. exploring only the base of a skills pyramid, which is the "knowledge". Some written tests may even assess "know how", but they do not allow us to evaluate the "show how to do it" and the practice itself, since these are skills that are at the top of the skills pyramid and that require more complex techniques to be evaluated.18 It is also important to mention that, although the instrument used for knowledge assessment was previously used with the same population, primary care workers, and a pre-test of the form was performed, it was not submitted to evaluation as to its psychometric properties.
The higher number of certification criteria met by the UBS after the intervention conducted in this study was consistent with the perception of managers regarding changes and with the number of CEA performed by the tutor, which are conducted with the very purpose of contributing to the certification process. The scope of the EAAB certification criteria reflects the change in the work process of the team, since it is determined by the confluence of several factors that include the realization and fulfillment of an action plan for the promotion of breastfeeding and CF, until the reorganization of child health care [4]. In addition, months after the end of the intervention, the municipality of Embu das Artes obtained the certification of five UBSs from the Ministry of Health.
Current EAAB implementation data in Brazil show that, in five years, 109 UBSs were certified, representing less than 5% of the trained UBSs, while in Embu das Artes in one year (including the intervention period), 38.5% of the UBSs were certified. These numbers strongly reinforce the validity of the findings of this study and the relevance of the Manual in the process of implementing EAAB.
A limitation of this study is that it does not allow an analysis of the influence of the use of the Manual on the skills and practices of workers related to nutritional counseling, one of the components of the intervention PIP. Although it is known that there are theories about the multiple factors that influence people's health behavior [19], the literature supports the understanding adopted in this analysis, that the best prepared workers are so not only in knowledge, but also in their counseling skills to the mothers, which could mediate the change in feeding practices of children. These studies found that educational interventions that provide training and prepare workers to promote infant feeding practices are able to qualify and strengthen nutritional counseling, which in turn improves the performance of health workers and nutritional outcomes in children, as well as promotes the adoption of healthy eating practices by caregivers [20-23].
Breastfeeding and nutrition counselling are known to be one of the most effective strategies for reducing the incidence of child morbidity and mortality [24]; however, there are many barriers related to this practice, already pointed out in the literature, such as knowledge deficits, difficulties regarding the practice of counseling and negative attitudes by the worker [21,25]. In this sense, it is considered that the proposal of the EAAB Tutor Support Manual meets the need to overcome these barriers through CEA that bring the perspective of counseling transversally when working on the following topics: clinical management of breastfeeding, promotion of healthy complementary feeding and communication skills with mothers and caregivers. However, to further clarify the ways and mechanisms by which the use of the Manual can impact child feeding practices, studies are needed to assess the immediate results in counseling practices.
In this sense, understanding the Manual as a tool to support the implementation of the EAAB, the ways and mechanisms of its use represented by the PIP is a potentiality of this study, since the possibility of answering how and why interventions produce their effects is a fundamental contribution to the reproducibility or external validity of interventions [26].
It is important to highlight that the use of the Manual has promoted changes mainly in the components that are located at the beginning of the PIP chain of mechanisms, those related to the knowledge and practices of tutors and health workers, demonstrating that they are sensitive indicators in the impact of the intervention and that they deserve to be considered in the evaluation of the use of the Manual in different contexts. The PIP diagram was useful to guide the evaluation of this study and can also be a tool to support managers in the process of implementation, monitoring and evaluation of EAAB [21,27].
Conclusion
The use of the Manual, by better preparing the tutor to conduct the continuing education process, is effective in improving the performance of health workers, who bring about changes in the work process, which is certainly reflected in the quality of counseling for mothers and can promote improvements in child feeding practices. The results of the evaluation of the intervention from the perspective of the tutors support these conclusions, since they revealed contributions of the use of the Manual in addition to the changes achieved in their technical knowledge. Thus, the findings of this study confirm the potential of the Manual and indicate the importance of its dissemination to all tutors, making it a support material for the implementation of EAAB.
Collaborators
Relvas GRB contributed to the conception and design, analysis and interpretation of the data, writing of the paper and critical review of the content and with the final approval of the version to be published. Buccini GS contributed with the analysis and interpretation of the data, critical review of the content and with the final approval of the version to be published. Venancio SI contributed with the conception and design, analysis and interpretation of the data, critical review of the content and with the final approval of the version to be published.
Acknowledgements
To the State Secretariat of Health of Mato Grosso and the Coordination for the Improvement of Higher Education Personnel. To the General Coordination of Food and Nutrition and the General Coordination of Child Health and Breastfeeding of the Ministry of Health. To the managers, tutors and primary care team of the Embu das Artes Municipal Health Secretariat; especially to Lucimeire Brockveld. Thanks to Louise Potvin of the University of Montreal-CA for her contributions to the study methodology. Special thanks to the journal Demetra for granting the copyright to this publication.
References
- Langley-Evans SC (2015) Nutrition in early life and the programming of adult disease review. J Hum Nutr Diet 28: 1-14.
- Victora CG, Bahl R, Barros AJD, França GVA, Horton S, et al. (2016) Breastfeeding in the 21st century: Epidemiology, mechanisms, and lifelong effect. Lancet 387: 475-490.
- Alvim NAT, Ferreira MA (2007) Perspectiva problematizadora da educação popular em saúde e a enfermagem. Texto Context Enferm 16: 315-319.
- https://bvsms.saude.gov.br/bvs/publicacoes/estrategia_nacional_promocao_aleitamento_materno.pdf
- Brandão DS, Venancio SI, Giugliani ERJ (2015) Association between the Brazilian Breastfeeding Network implementation and breastfeeding indicators. J Pediatr (Rio J) 91: 143-151.
- Venancio SI, Martins MCN, Sanches MTC, Almeida H, Rios GS, et al. (2013) Análise de implantação da Rede Amamenta Brasil: Desafios e perspectivas da promoção do aleitamento materno na atenção básica. Cad Saude Publica 29: 2261-2274.
- Denis JL, Champagne F, AnáliseDI, In Hartz ZMA (1997) Avaliação em saúde: Dos modelos conceituais à prática na análise da implantação de programas. Rio de Janeiro: Fiocruz 49-88.
- Yin RK (1994) Case Study Research: Desing and methods. Thousand Oaks, CA: Sage Publications.
- http://tabnet.datasus.gov.br/cgi/tabcgi.exe?cnes/cnv/equipern.def
- Kim SS, Habicht JP, Menon P, Stoltzfus RJ (2011) How do programs work to improve child nutrition? IFPRI Discuss 44.
- Rawat R, Nguyen PH, Ali D, Saha K, Alayon S, et al. (2014) Learning how programs achieve their impact: Embedding theory driven process evaluation and other program learning mechanisms in Alive & Thrive. Food Nutr Bull 34: 212-225.
- Rogers PJ (2000) Program theory Not whether programs work but how they work. In Evaluation Models SDI MFG KT Boston Kluwer Academic 209-232.
- Buccini G, Harding KL, Fiedler AH, Escamilla RP (2014) How does Becoming Breastfeeding Friendly work A Programme Impact Pathways Analysis 1-13.
- Toma TS (2008) Alimentação de crianças do Programa Saúde da Família (PSF) fatores associados à amamentação plena e impacto de um curso de aconselhamento em alimentação infantil nos conhecimentos de trabalhadores da saúde.
- Bardin L (1977) Análise de conteúdo Lisboa Edições.
- Miccas FL, Batista SHS (2014) Educação permanente em saúde: Metassíntese. Rev Saúde Pública 48: 170-185.
- Maia ER, Junior JFL, Pereira JS, Eloi AC, Gomes C, et al. (2012) Educational Technologies for Child Health Promotion: An Integrative Literature Review. Rev nutr 25: 79-88.
- Wass V, Vleuten CV, Shatzer J, Jones R (2001) Assessment of clinical competence. Lancet 357: 945-949.
- Rothman AJ (2004) Is there nothing more practical than a good theory Why innovations and advances in health behavior change will arise if interventions are used to test and refine theory. Int J Behav Nutr Phys Act 1:11.
- Bhandari N (2015) Use of multiple opportunities for improving feeding practices in under twos within child health programmes. Health Policy Plan 20: 328-336.
- Campos AAO, Cotta RMM, Oliveira JM, Santos AK, Araujo RMA (2014) Aconselhamento nutricional de criancas menores de dois anos de idade potencialidades e obstaculos como desafios estrategicos. Cien Saude Colet 19: 529-538.
- Coutinho SB, Lira PI, Lima MC, Frias PG, Eickmann SH, et al. (2014) Promotion of exclusive breast-feeding at scale within routine health services impact of breast feeding counselling training for community health workers in Recife Brazil. Public Health Nutr 17: 948-955.
- Vitolo MR, Rauber F, Dal P, Campagnolo B, Feldens CA, et al. (2010) Maternal Dietary Counseling in the First Year of Life Is Associated with a Higher Healthy Eating Index in Childhood. J Nutr 140: 2002-2007.
- Bhutta ZA, Ahmed T, Black RE, Cousens S, Dewey K, et al.(2008) What works Interventions for maternal and child undernutrition and survival. Lancet 371: 417-440.
- Laantera S, Polkki T, Pietila AM (2011) A descriptive qualitative review of the barriers relating to breast feeding counselling. Int J Nurs Pract 17: 72-84.
- Oliveira LGD, Natal S, Felisberto E, Alves CKA, Santos EM (2010) Modelo de avaliação do programa de controle da tuberculose. Cien Saude Colet 15: 997-1008.
- PérezEscamilla R, SeguraPérez S, Damio G (2014) Applying the Program Impact Pathways (PIP) evaluation framework to school based healthy lifestyles programs Workshop Evaluation Manual. Food Nutr Bull 35: S97-S107.
Citation: Relvas GRB, Buccini GDS, Venancio SI (2022) Evaluation of the use of a manual to support a large-scale implementation of the Estratégia amamenta e alimenta Brazil. J Food Sci Nutr 8: 143.
Copyright: © 2022 Glaubia Rocha Barbosa Relvas, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.