Financial and Geographic Barriers in Seeking and Utilizing Eye Healthcare in Bangladesh
*Corresponding Author(s):
Md Mahmudul HasanDepartment Of Research, Education And Training, Al-Noor Eye Hospital,(Al- Basar International Foundation) 1207, 1/9 E Block, Satmasjid Road, Lalmatia, Dhaka, Bangladesh
Tel:+8801 712079513,
Email:mahmud.albasar@gmail.com
Abstract
Background: Eye diseases are quite prevalent across the world. Like any other low and middle income countries (LMIC), population in Bangladesh also suffers from various eye diseases. The eye healthcare seekers in Bangladesh are often deprived of accessing or utilizing eye care services for various personal, financial, geographic, resource and service related obstacles. This study had focused on financial and geographic barriers in accessing eye health care services to make relevant policy recommendations.
Methodology: A desk review on literature published between 2000-2021 using the keywords “barriers”, “costs”, “eye”, “eye services”, “vision health” “eye health” and “Bangladesh” was performed to find out research papers on financial and geographic barriers in accessing, and utilizing eye care services in Bangladesh. Pubmed, Google Scholar, and Bangladesh Journals Online (BanglaJoL) were the primary sources of databases used in this study.
Results: The expenses associated with diagnosis, registration, medications, continuing care, hospitalization, transportation, food, and accommodation were identified as major financial barriers for eye patients. On the other hand, location of eye care service facilities requires long travel time along with long distances to cross and these created geographical barriers in receiving eye care.
Conclusion: Measures that may increase accessing and utilizing eye health care may include introduction of health insurance covering fully or partially eye healthcare, spectacles and common eye surgeries and medicines and subsidize medical travel expenses; setting up of small satellite eye clinics, offering eye care services at Upazilla level clinics, offering tele-ophthalmology in underserved areas, providing incentives for eye doctors to practice in remote areas.
Keywords
Eye; Eye healthcare; Barriers; Financial barriers; Geographic barriers; Bangladesh
Introduction
The World Health Organization (WHO) estimates that about 2.2 billion people have visual impairment globally due to eye diseases that include presbyopia (1.8 billion), refractive error (123.7 million), cataract (65.2 million), age-related macular degeneration (10.4 million), glaucoma (6.9 million), corneal opacities (4.2 million), diabetic retinopathy (3 million), trachoma (2 million), and other eye disorders (37.1 million) [1]. Of the global visual impairment, about 90% is reported to occur in low and middle income countries (LMIC) [2]. In Bangladesh- a major LMIC with more than 160 million people - there are over 6 million people who are reported to be visually impaired and another 0.75 million are reported blind according to a 2019 estimate [3]. According to WHO, about 80% of visual impairments such as loss of central and side vision, blurred vision, generalized haze, light sensitivity of eye, night blindness and blindness cases can be prevented with adequate and timely eye care [2] which may not be the case for many chronic diseases. Unfortunately, eye health services in Bangladesh and many other LMICs are scarce, costly, are not always easily accessible or there is less awareness or knowledge in the general population about the preventative and curative measures. At the same time eye health services are given low priority from the policy makers’ perspectives and thereby receive little attention and healthcare resources.
Research suggests that a substantial portion of eye patients in LMIC as well as in developed countries tend to not use eye health services, even when these are available [4,5]. Financial, geographic, attitudinal, awareness and service related factors have been identified as barriers for not utilizing eye care by some previous authors [4-7]. Little attempts have been put together to identify and report on these barriers in Bangladesh that has high prevalence of eye disease and associated social and economic burden. Barriers identified in other countries particularly in the developed countries may not be similar and comparable to Bangladesh because of its unique socio-cultural norms, demographic characteristics and economic conditions of the population which are compounded by the fact that eye care facilities and provisions are quite scarce or inadequate compared to its very large population size. There may also be country specific barriers in seeking and utilizing eye care which if not correctly catalogued or described, policy options to address these will remain misdirected or suboptimal.
Among the categories of barriers, financial and geographic can be grouped together as causes and policy measures for addressing these barriers are different from the attitudinal or awareness barriers which may need long term educational programs and awareness building efforts focusing on improving the general and health-related literacy of the population, changing socio-cultural view of looking at eye problems less seriously as non-life threatening health issues whereas the service related barriers or factors relate to quality of patient care provided, training and skills development as well as supply of eye care providers, creating better diagnosis and treatment provisions, etc. This research investigation focused on the financial and geographic barriers.
For an LMIC country with per capital GDP of $ 1968.79 [8] and 20.5 % people still living below poverty line [9], out of pocket costs are the immediate and major barriers in seeking and accessing healthcare services including eye related care. Spending on healthcare in general is very low from both the individual citizen as well as government’s perspective. Economically struggling citizens identify food, accommodation, and clothing as high priority needs and few people are willing to spend their earnings or savings for seeking preventive eye care and may only seek care for it when the issue is acute or become severe. Accessing eye health services cost money despite Bangladesh’s publicly funded primary healthcare delivery system: from reaching the hospital-which is often far away to paying for the fees for doctor consultation, medication, diagnosis, tests and treatment in addition to bearing other associated costs such as accommodation and meals for the patients and accompanying caregivers; all of these may become a hefty amount creating undue burden for anyone beneath the middle and upper social class in this country.
Conversely, geographic barriers may prevent people from reaching eye healthcare facility even when the financial barrier is not the primary concern. The location of a facility may distract a care recipient as Bangladesh has in general a fragmented and very slow transportation network; travelling to any distance takes a very long time because of poor quality of vehicles and deplorable road conditions along with persistent traffic jam countrywide. On the other hand, shabby compartments, dirty toilets, long delays, unfriendly-access to stations and platforms, ticketing mismanagement, and lack of security have made the railway transportation unattractive for a lot of people. A major portion of the population depends on waterways and a large part of the country goes under water for almost half of the year. Water transportation is slower than road or rail in general. Around 3,800 km of year round navigable waterways with 6,000 km additional navigable water ways in the rainy season in Bangladesh make people depend on traveling by water transportation mode [10]. Access to an eye care hospital- be it public or private-often depends on its location and proximity.
This comprehensive review is conducted to compile updated evidence on financial and geographic barriers in accessing and utilizing eye care services in Bangladesh. By summarizing findings from published research studies on barriers, this study may help understand the extent and root causes of such barriers so that attention and awareness can be created among the government policy makers and other eye health stakeholders and thereby helps prioritize eye care access issues. The evidence may help develop and implement interventions and programs to reduce the prevalence and burden of eye diseases and conditions in Bangladesh and other LMICs.
Methodology
A literature review was conducted to find out studies on Bangladesh that covered financial and geographic barrier issues on eye healthcare services. PubMed and Google Scholar were the major sources; in addition, Bangladesh Journals Online (BanglaJOL) that include local journals that may not be peer reviewed or indexed in international scholarly databases was also consulted. Search items included: “barriers”, “costs”, “eye”, “eye services”, “vision health” “eye health” along with “Bangladesh”. The search was limited to articles published between 2000-2021.
All the articles were carefully reviewed; their titles and abstracts were read first to find out relevance. The full texts were then retrieved and findings were summarized. The barriers addressed or highlighted were categorized. Definitions and details of these barriers were presented and when available the exact results and methods of measurements were synthesized and interpreted. In reporting on the financial and physical barriers, this study took the patients’ perspective. Further, additional studies were retrieved and consulted to list the cost categories and operationally define these as well as to provide a summary of methods used previously in reporting these common cost categories.
Results
A total of 5 published studies (Table 1) were found in this literature search. Of these, only one was directly addressed the barrier issue. The rest were not directly related to barriers; however; their findings provided barrier related information to some extent.
During literature search, the researchers found that most of the studies focused on reporting of prevalence of eye diseases and described the socio-demographic profile of the patients while some have addressed the effectiveness of clinical interventions and management while few others covered topics like knowledge, attitude and practice on eye diseases. Five research articles looked at the influencing factors, patients’ satisfaction and mode of delivery of eye health services [11-15] which were found to be relevant to this review to understand and describe the barriers and they helped to develop the conceptual framework used in this study. Table 1 provides the details on these studies.
|
Study; method; population |
Purpose |
Major findings |
Emerged theme |
|
Sarker et al. [11]; 5000 eye care facilities were mapped and assessed; 1,600 randomly selected individuals over 18 years were surveyed; 558 patients from 5 selected eye care facilities including a mix of public and NGO facilities were interviewed;28 participants evenly divided in 4 Focus groups were interviewed |
To better understand the demand and provision of eye care services in Dhaka with a specific focus on urban slum-dwelling communities. |
About 38% of respondents did not seek any eye treatment ever. Of these, 45% mentioned financial hardship as the reason for not seeking eye care. Other reasons included taking the problems lightly and lack of time which were mentioned by 31% and 16% of participants, respectively. |
Financial, awareness/ attitude |
|
Alam [12]; 410 children were clinically examined and an equal number of their parents were interviewed to collect health-seeking behaviors and identify barriers. |
To find out the ocular status, health seeking behaviors and barriers to uptake eye care services among children of slum community in Chittagong, Bangladesh |
Most of the respondents (73%) had never seen an eye care doctor because of their parents’ poor economic condition. |
Financial |
|
Das et al. [13]; The data was collected from the International Agency for Prevention of Blindness (IAPB) country chairs and included information regarding the national health policy, national health expenditure, insurance and out of pocket expense for eye health care, the strength of eye health personnel, training and future man power planning and presence of the international non-governmental organization (INGO).
In addition, it also accessed the PubMed referenced articles using the key words ‘‘blindness,’’ ‘‘low vision,’’ ‘‘vision impairment,’’ ‘‘south east Asia’’ from January 2000 to December 2015. |
The status of eye care service data and profile in Southeast Asia countries was compared between 2015 and 2010 to determine the state of preparedness to achieve the World Health Organization global action plan 2019. |
In Bangladesh, several challenges existed for the rural people to access quality eye care services due to cost and distance. There is no universal health insurance scheme in the country. Out-of-pocket expense for healthcare or eye care is over 90%. |
Financial, geographic |
|
Ferdausi et al. [14]; 20 In-depth-interviews (IDIs) among policymakers, eye care managers, and service providers, and 4 FGDs among parents in the public hospitals’ and private chambers’ eye care facilities, and another 2 FGDs among schoolteachers were carried out. |
To elucidate factors that influence, positively or negatively, people's willingness to seek and utilize pediatric eye care services |
Non-availability, poor accessibility of services, non-affordability, poor knowledge of available services have been identified that prevent parents from using eye care services for their children |
Financial, service related, awareness/ attitude, geographic. |
|
Quddus et al. [15]; A survey among 300 patients from three departments-outdoor, indoor, and postoperative was conducted. |
To assess the level of satisfaction of patients with the services received at the outpatient department and indoor patient department of an eye hospital of Chittagong city in Bangladesh. |
Patients had to wait for 4.3 hours on an average at the outdoor services and 5 hours at the post-operative services. The study indicated that 74% outdoor and 83% postoperative patients travelled 67 km on average to reach the facility. |
Geographic, service related. |
Table 1: Major findings and emerging themes from a review of studies on eye care service studies in Bangladesh.
Financial barriers
A study on access to public healthcare facilities in Bangladesh found that the use of the services there requires spending money for medicines, doctor's advice, hospitalization, and examination / investigation as well as there are costs of transportation and wage lost for the day off from work to reach healthcare facilities [16]. In other words, direct or indirect costs are involved to use health services even at public facilities. Another survey based study from Bangladesh broadly divided healthcare costs into three headings: direct medical costs, direct non-medical costs, and indirect costs [16]. Table 2 presents the details on these cost categories.
|
Direct medical cost |
Diagnosis-costs incurred during diagnosing an eye problem. Registration fees-costs of doctor consultations and follow up visits. Medications- costs incurred for prescription medicines and supplies after consultation. Continuing care- costs arising from use of aids or equipment; Hospitalization- fees to pay if in patient stay was required [17]. |
|
Direct non-medical cost |
Transportation-costs incurred for coming to the facility. Housing- costs required for accommodation of the patient and/or caregiver and food costs-costs to pay for the meals of the patient and/or caregiver [18,19]. |
|
Indirect cost
|
This refers the monetary value of a patient or family caregiver’s income lost related absences from work due to illness or treatment (both paid and unpaid) [17]. Unpaid work- it means the work that produces goods and services but which carries no direct remuneration or other form of payment like housework and care work. Paid work- it means the work done for payment or in expectation of payment and does not include being engaged by a charitable or voluntary organization or as a volunteer. |
Table 2: Cost Categories, definitions and examples.
Prior authors looked at the cost spending on different purpose in order to seek eye care services in Bangladesh. These costs could be fallen into different themes like spectacles, cataract surgery, phacoemulsification, medicine among rural and urban patients, Out of pocket health care expenditure, average travel expenses, food and accommodation and so on. Distribution of these expenditure to access and use eye care in Bangladesh is illustrated in table 3.
|
Category of cost and reference |
BDT (USD) |
Method of Estimation |
|
A pair of spectacles [11] |
597 (7.23$) |
Respondents’ willingness to pay (WTP) for spectacles were elicited as part of the interview. |
|
Small incision cataract surgery (SICS) [20] |
7,579 (89.16$) |
A structured questionnaire was developed to elicit willingness to pay (WTP) for SICS and Phacoemulsification. |
|
Phacoemulsification [20] |
10,208 (120.09$) |
|
|
Cost of medicine among rural patients [21] |
1078 (12.68$) |
A total of 12 400 patients who had paid to receive any type of healthcare services within the previous 30 days were analyzed from the Bangladesh Household Income and Expenditure Survey data, 2010. |
|
Cost of medicine among urban patients [21] |
2045 (24.06$) |
|
|
Out of pocket health care expenditure [21] |
2351(27.66$) |
|
|
Average travel expenses incurred by clients to travel to District Hospitals [16] |
87 (1.02$) |
Through face to face interview. |
|
Food and accommodation [16] |
383.11 (4.5$) |
|
|
Average transportation cost for public hospitals in urban areas [17] |
83.3 (0.98$) |
Direct interview physically.
|
|
Average transportation cost for private hospitals in urban areas [17] |
50 (0.59$) |
|
|
Patients’ income loss (Public hospital) [17] |
9643 (128.59$) |
|
|
Patients’ income loss (Private hospital) [17] |
5338 (71.18 $) |
|
|
Cost for shared rooms at public hospitals [22] |
150 (1.76$)
|
Reviewing revenue and expenditure of the Government of Bangladesh regarding health services. |
|
Cost for individual rooms at public hospitals [22] |
600 (7.05$) |
Table 3: List and estimation of costs to access and use eye care in Bangladesh (Description of costs estimated previously by different studies).
These cost categories were reported before in burden of illness and disease studies and have been considered here to develop a diagram on financial barriers (Figure 1).
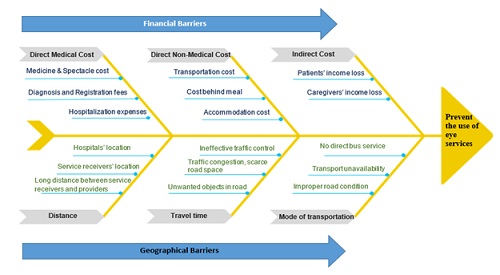 Figure 1: Financial and geographical barriers in utilization of eye care services.
Figure 1: Financial and geographical barriers in utilization of eye care services.
Geographical barriers
A barrier is geographical when the distance between the care recipient and care provider is big and other associated factors make the travel difficult, inconvenient, lengthy, or costly. National Health Service (NHS) of Great Britain identified long distance, and transport issues as the geographical barriers of a health delivery system [20]. Long distance needs more travel time, particularly when the road is not in good condition, traffic is slow or crowded with a large number of vehicles. On the other hand, ease of transport also depends on the quality and availability of vehicles be it via road, rail or water. Therefore, distance, travel time, mode of transport, and quality and availability of vehicles are discussed here briefly as geographical barriers of utilizing eye care services in Bangladesh.
Distance
A survey on eye care services at a tertiary hospital in Bangladesh found that about 74% and 83% of outdoor and postoperative patients had to travel 67 km on average respectively to reach the hospital [21]. Similarly, another research pointed out 70 km as the maximum distance traveled by the health service seekers to reach a care providing institute in Bangladesh [23].These results are generalizable as eye care is provided only in district secondary level hospitals in Bangladesh [24]. Further, there are only two government tertiary level eye hospitals in the country situating in Dhaka and Gopalganj which leaves patients with severe eye complications who cannot afford private and costly treatment no other choice but to travelling a huge distance. As a result of this long distance travel requirement, access to quality eye care services has been reported to be delayed or impossible by previous authors [4,13].
Travel time, mode of transport and transportation issues
A study on outpatients attending public and private hospitals in Bangladesh reported that the average travel time to the public and private hospitals is 75.59 and 44.14 minutes, respectively [17]. This data signifies that patients require more time reaching the public than private hospitals in Bangladesh since there are less public hospitals [25]. Eye service is usually delivered at the district level hospitals for patients with mild to moderate conditions, and the two public tertiary level hospitals provide services to patients with chronic or complex eye diseases. This suggests that compared to other common diseases or conditions, patients with eye diseases require more travel time to receive treatment from public health facilities. In addition to distance, travel time depends on the traffic congestion which can be notorious in the city areas. For example, a person can only pass 7 km in an hour through traffic congestion in Dhaka [26]. Moreover, there is a lack of an adequate number of public transportation in the urban areas of Bangladesh. On the other hand, large sections of rural roads become inaccessible during the rainy season, and inadequate public transport and interrupted transport routes, make travel time too long towards eye seeking health services. Long trips needed for getting eye services may lead to treatment withdrawal or negligent behavior that may eventually prevent receiving timely eye treatment and deteriorate the eye condition, eventually making the recovery difficult or impossible.
Discussion
This review study summarized existing evidence on financial and geographical barriers to eye care services in Bangladesh from the patient perspective to gain an in-depth understanding of the issues as well as to advise policymakers on possible interventional programs to mitigate some of these barriers.
Being an LMIC with a GDP per capita of $ 1968.79 in 2021 [8], it is difficult for the majority of the Bangladeshi population in general to afford the treatment cost for any disease. Public hospital in Bangladesh government healthcare sector provides free treatment for all patients and 50 percent discount on medicines [22,27]. But drug unavailability and poor functioning of medical devices and instruments are very common scenario at public health facilities in Bangladesh [24]. The absence of these services in public hospitals force eye healthcare candidates to move to nearby private hospitals. In addition, there is no provision for free spectacles in government hospitals though eye surgeries are performed for a small fee. A study revealed that the cost of services (laboratory cost, surgery cost, and Doctor’s consultation fee) in private hospitals is much higher in Bangladesh [28]. Evidence suggest that due to the high cost, people with low income may fail to afford spectacles and refrain from examining eyes or performing surgery [29,30]. In contrast, a previous study shows that the provision to reduce the cost of eye surgery increases the number of cataract surgery [31], and the health insurance that covers the cost of eye services reflects the behavior of seeking eye health [32]. Therefore introducing a public health insurance scheme that includes eye health care in Bangladesh should be taken seriously. Along with this, provisions for low-cost spectacles and making eye care services more affordable reflecting the purchasing power of the majority of the common people by the government may help improve eye healthcare in Bangladesh. With regards to increasing the uptake of surgery, policymakers should allocate more budgets to subsidize eye surgery in public and private eye hospitals, and charities or national and international non-government agencies may actively expand their coverage to meet the eye surgery needs of low- and middle-income groups in the country particularly those living in remote areas.
The overwhelming majority of patients have to travel a long distance to get appropriate treatment when they suffer from chronic diseases in Bangladesh. Long-distance travel for treatment brings in financial constraints [33]. In Bangladesh, approximately 70% of the workforce lives in rural areas and two-third of them are directly involved in agriculture [34]. The annual family income of the farmers who depend on agriculture is about annually Tk. 2, 02,724 (2384.50 $) or monthly Tk. 16,893 (198.70 $) [35]. Based on the international poverty line definition (earning below 1.90 dollars per day), 20.5% of people of Bangladesh live under the poverty line that means monthly they earn lower than Tk. 4,833 (56.85$) [9]. According to another report, the average treatment cost in public hospitals for outpatients including direct and indirect costs is Tk. 9,923 (116.74$) in Bangladesh [17]. This cost is much higher for hospitalized or inpatient patients because a survey found that a patient spends (including direct and indirect cost) around Tk 24,898 (290$) in a government hospital in this country [19]. However, out-of-pocket spending varies greatly with the disease and its severity. Since there is no study about out of pocket expenditure on eye diseases in Bangladesh, therefore, future research can investigate and report on this.
Long travel time was considered as the burden for health care seekers by a research conducted by Sarnquist et al., [36]. In addition, prior authors argued that long distances and lack of transportation not only create barriers to regular eye check-ups, but also impede the proper management of other diseases such as diabetes that can cause eye diseases [37,38]. One study in India showed that subsidization of travel costs resulted in a significant increase in the utilization of cataract surgery [31]. This suggests commencing of transport-related subsidies for eye care patients. In addition, the eye health service providers should try to reach all the potential eye patients by setting up satellite eye clinics in underserved communities where eye specialists would provide services at least once a week from the nearby institute. Moreover, the introduction of telemedicine based eye healthcare services may increase the accessibility of doctor consultation. Besides, the ministry of health may offer incentives for relocation of doctors to primary health care centers located in rural areas, so as to reduce the distance, travel time, and transportation cost for providing eye related services.
Conclusion
In Bangladesh, a large number of people are visually impaired and blind, and twice as many people are at risk of being visually impaired or blind due to eye diseases. Proper, timely, and regular eye checkups play a big role in preventing and curing vision-related diseases. In Bangladesh, eye patients incur the expenses of spectacles, surgery, medicine, transportation, food, accommodation, as well as they have earning loss and all of these create financial barriers. Distance, travel time, mode of transport, and transportation issues act as geographical barriers in utilizing eye care facilities. Introducing health insurance including eye health provisions, subsidizing medical related travel and surgery costs, arranging of low cost accommodation, and option for cheaper meal or catering services may help lessen financial burden among eye health candidates. On the other hand, geographical barriers could be reduced if public and private hospitals expand their service coverage area with the establishment of satellite clinics and introduce tele-ophthalmology services to the underserved areas. In addition, placement of more ophthalmologists with incentives to the rural areas could prevent eye healthcare seekers from traveling long distances to receiving eye health services.
Conflict of Interest
None
Acknowledgement
The authors would like to thank the authority of Al Noor Eye Hospital, Dhaka, Bangladesh (run by Al-Basar International Foundation) for providing the support during carrying out this research.
References
- World Health Organization (2021). World Report on Vision. World Health Organization, Geneva, Switzerland.
- World health organization - eastern Mediterranean region (2021) Control and Prevention of Blindness and Deafness. World Health Organization, Geneva, Switzerland.
- The Daily Star (2021) Six million Bangladeshis visually impaired: speakers. The Daily Star, UK.
- Chou CF, Sherrod CE, Zhang X, Barker LE, Bullard KM, Crews JE, et al. (2014) Barriers to eye care among people aged 40 years and older with diagnosed diabetes, 2006-2010. Diabetes Care 37:180-188.
- Unite for Sight (2021) Patient barriers to eye care - community eye health course. Unite for Sight, USA.
- Palagyi A, Ramke J, du Toit R, Brian G (2008) Eye care in Timor-Leste: a population-based study of utilization and barriers. Clin Experiment Ophthalmol 36:47-53.
- Akowuah PK (2017) Barriers to utilization of eye care services in the upper east region, Ghana. Advophthalmolvissyst 7:62-65.
- World Bank (2021) GDP per capita (current US$) – Bangladesh. World Bank, Bangladesh.
- Asian Development Bank (2021) Poverty: Bangladesh. Asian Development Bank, Bangladesh.
- Valentine H (2021) The Bangladesh commercial river transport industry Maritime-executive.com. The Maritime executive, Bangladesh.
- Sarker M, Rabbani A, Engels T, Gayen P, Islam MN, et al. (2021) Understanding demand and provision of eye care services among slum-dwellers in Dhaka, Bangladesh. JPC, Bangladesh.
- Alam SMD (2021) Ocular status, health seeking behaviors and barriers to uptake eye care services among children of slum community in Chittagong, Bangladesh. J Clin Exp Ophthalmol 8: 6.
- Das T, Ackland P, Correia M, Hanutsaha P, Mahipala P, et al. (2018) Is the 2015 eye care service delivery profile in Southeast Asia closer to universal eye health need! Int Ophthalmol 38: 469-480.
- Ferdausi N, Khan J, Khan T (2021) Factors influencing utilization of pediatric eye care services in bangladesh: a qualitative study. Acta Scientific Ophthalmology 4: 116.
- Quddus AGH, Islam MS, Uddin M, Osmani M, Gupta JD (2013) Patients’ satisfaction with eye care services in a tertiary hospital of Bangladesh. A Journal of Institute of Community Ophthalmology and Chittagong Eye Infirmary & Training Complex 8: 1-8.
- Mannan MA (2013) Access to public health facilities in Bangladesh: a study on facility utilization and burden of treatment. Bangladesh Development Studies XXXVI: 25-80.
- Pavel MS, Chakrabarty S, Gow J (2016) Cost of illness for outpatients attending public and private hospitals in Bangladesh. Int J Equity Health 15:167.
- Ibrahim N, Pozo-Martin F, Gilbert C (2015) Direct non-medical costs double the total direct costs to patients undergoing cataract surgery in Zamfara state, Northern Nigeria: a case series. BMC Health Serv Res 15: 163.
- Haque MF, Islam AS, Pervin S, Akter E, Hasan MM (2021) Catastrophic health expenditure, distress financing and impoverishment due to out-of-pocket expenses for healthcare among patients with chronic liver disease: A cross-sectional study among hospitalized patients in Bangladesh. Lancet 4: 1.
- Islam MN, Engels T, Hossain S, Sarker M, Rabbani A (2019) Willingness to pay for cataract surgeries among patients visiting eye care facilities in Dhaka, Bangladesh.Appl Health Econ Health Policy 17: 545-554.
- Mahumud RA, Sarker AR, Sultana M, Islam Z, Khan J, et al. (2017) Distribution and determinants of out-of-pocket healthcare expenditures in Bangladesh. J Prev Med Public Health 50: 91-99.
- World Health Organization (2021) Bangladesh Health System Review. World Health Organization, Geneva, Switzerland.
- Castlefordacademy.com (2021) What are barriers? Castlefordacademy.com, Bangladesh.
- ORBIS (2021) Eye care in Bangladesh. ORBIS, Bangladesh.
- Dhaka Tribute (2021) Private healthcare facilities growing in number, but lack emergency services. Dhaka Tribute, Bangladesh.
- The Daily Star (2021) Traffic jam: The ugly side of Dhaka's development. The Daily Star, Bangladesh.
- Justice Gov (2021) Bangladesh: Medical and Healthcare issues. Justice Gov, Bangladesh.
- Siddiqui N, Khandaker SA (2007) Comparison of services of public, private and foreign hospitals from the perspective of Bangladeshi patients. J Health Popul Nutr 25: 221-230.
- Hodges LE, Berk ML (1999) Unmet need for eyeglasses: results from the 1994 Robert Wood Johnson Access to Care Survey. J Am Optom Assoc 70: 261-265.
- Nishad N, Hewage SA, Arulmoly K, Amaratunge MS, Silva JD, et al. (2019) Barriers for cataract treatment among elderly in Sri Lanka. Curr Gerontol Geriatr Res 2019: 6262456.
- Ellwein LB, Lepkowski JM, Thulasiraj RD, Brilliant GE (1991) The cost effectiveness of strategies to reduce barriers to cataract surgery. The Operations Research Group. IntOphthalmol 15: 175-183.
- Harmon C, Nolan B (2001) Health insurance and health services utilization in Ireland. Health Econ 10: 135-145.
- Tadesse T, Demissie M, Berhane Y, Kebede Y, Abebe M (2013) Long distance travelling and financial burdens discourage tuberculosis DOTs treatment initiation and compliance in Ethiopia: a qualitative study. BMC Public Health 13: 424.
- World Bank (2021) Bangladesh: Growing the economy through advances in agriculture. World Bank, Bangladesh.
- TBS News (2021)Agriculture not main income source of farmers. TBS, Bangladesh.
- Sarnquist CC, Soni S, Hwang H, Topol BB, Mutima S, et al. (2011) Rural HIV-infected women’s access to medical care: ongoing needs in California. AIDS Care 23: 792-796.
- Owsley C, McGwin G, Scilley K, Girkin CA, Phillips JM, et al. (2006) Perceived barriers to care and attitudes about vision and eye care: focus groups with older African Americans and eye care providers. Invest Ophthalmol Vis Sci 47: 2797-2802.
- Strauss K, MacLean C, Troy A, Littenberg B (2006) Driving distance as a barrier to glycemic control in diabetes. J Gen Intern Med 21: 378-380.
Citation: Hasan MM, Chowdhury IH, Hamid SAT, Alamgir HM (2023) Financial and Geographic Barriers in Seeking and Utilizing Eye Healthcare in Bangladesh. J Ophthalmic Clin Res 10: 109.
Copyright: © 2023 Md Mahmudul Hasan, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.