Good Life Project: Description of the Impact of Weight Loss Intervention at a Private Health Service in Manaus
*Corresponding Author(s):
Caroline Souza Dos AnjosClinical Oncologist, Sensumed Oncologia, Manaus, Amazonas, Brazil
Tel:+55 09221295675,
Email:carolinesanjos@gmail.com
Abstract
Introduction
Cardiovascular diseases, followed by neoplastic diseases and complications of diabetes, are among the major causes of death worldwide. All of them are directly related to the life style of most of the population. Today it is know that weight loss contributes to the reduction of the incidence of these diseases.
Objective
To describe the impact of weight loss intervention for the promotion of health at a private oncology clinic in Manaus-AM.
Patients and methods
This was a longitudinal, prospective, observational and descriptive study conducted on 41 employees of Sensumed Oncologia.
Results
36 patients were weighed in the first and 6th month of the study, with a 1.08 to 19.34%, weight loss for a total amount of 43.74kg. A total of 72.22% of the subjects practice regular physical activity, with 30% of them starting to do during the project. The greatest impact on laboratory tests was a reduction of the lipid profile, although there was also a discrete reduction of fasting glycemia in both sexes without pharmacological measures. Bioimpedance revealed a modest reduction of fat mass.
Conclusion
A more intensive intervention regarding health promoting activities is necessary, mainly where large part of the population spends most of the day in the workplace. Thus, it is possible to prevent obesity, a serious public health problem, thus reducing the morbidity and mortality of the population and the incidence of this important risk factor for the onset of chronic diseases.
Keywords
Healthy diet; Physical activity; Weight loss
INTRODUCTION
Over the last decades, overweight and obesity have become one of the greatest public health problems worldwide. Previously affecting exclusively developed countries, this problem now affects also developing countries such as Brazil. The projection is that, by 2025, about 2.3 billion adults will be overweightin the world and that more than 700 million people will be obese. This alarming result has been related to high calorie intake, to the reduction of time destined to phyisical exercise, sleep deprivation, and mental factors such as depression and anxiety [1].
To conceptualize overweight and obesity, the World Health Organization (WHO) uses the Body Mass Index (BMI). This classifies as overweight people with a BMI of 25 to 29.9kg/m² and obesity as people with a BMI over 30kg/m². Because it is simple to apply and cost-effective, BMI is still the most widely used method, but it has limitations, such as not differentiating fat from lean mass. Electrical bioimpedance seems to try to minimize this body fat analysis bias because it examines body composition individually: body fat, visceral fat, basal metabolism, skeletal disorders muscles, age and body water [1,2].
Overweight and obese people have a higher risk of morbidity due to hypertension, type 2 diabetes, dyslipidemia, coronary artery disease, heart attack, respiratory diseases, osteomuscular diseases, and neoplasias. In addition, there is also an increase in mortality due to cardiovascular disease among overweight people. In order to reduce the prevalence of excess weight and the complications related to this global epidemic, it is necessary to implement health promotion and preventive measures with the adoption of healthy life habits [1,3-6].
The two main factors for weight loss are undoubtedly a healthy eating associated with exercise. According to the Brazilian Society of Diabetes, 7% weight loss combined with 150 minutes of moderate physical activity or 75 minutes of vigorous weekly physical activity results in reduced risk of diabetes in prediabetic or overweight patients. According to the Brazilian Society of Cardiology, overweight reduction, regular exercise and healthy eating are essential for the prevention and control of cardiovascular disease. And finally, the National Cancer Institute (INCA) states that overweight is strongly related to the risk of developing 13 different cancers [7-9].
There is an urgent need for interventions on the part of health professionals in order to modify this unfavorable outcome that results in a reduced quality of life and life expectancy and in increased health costs for the treatment of diseases secondary to excess weight. Many studies have reported positive results after interventions involving public policies and the monitoring of people for a given period of time, with the implementation of actions such as weight monitoring and laboratory tests, health promotion campaigns, encouragement of the regular practice of physical exercises, and the adoption of a healthy diet [10-12].
Thus, in view of the above considerations, Sensumed Oncologyhas created the Goord Life project, applied to its staff in order to encourage weight loss by means of lectures with dietary guidelines and with emphasis on the importance of regular physical exercise.
MATERIALS AND METHODS
A longitudinal, prospective, observational and descriptive study was conducted on 41 employees of Sensumed Oncologia, who represent the entire administrative (23), nursing (4), medical physicist (2), radiotherapy and chemotherapy’s technical area (9), and general services staff (3). Exclusion criteria were: employees who a) had been admitted after the beginning of the project, b) had left the clinic during the follow-up period, c) were pregnant or had become pregnant during the course of the project, d) did not perform the laboratory exams and/or bioimpedance during the months initially planned.
The professionals of Sensumed Oncologia included in the study were first contacted in a doctor’s office by the investigators,where they were informed about the methodology and objectives of the investigation and gave written consent to participate in the study.
Body Mass Index (BMI) was calculated and analyzed according to sex using the body weight and height measured during the initial visit and in the 6th month of the study using aWelmy W200/5 scale with a 200kg measuring capacity. Bioimpedance was performed in the initial month and in the 6th month of the study using a tetrapolar single frequency Biodynamics analyzer, model 450. Laboratory tests were performed in the initial month and the 6th month by the Santa Clara laboratory (Manaus-AM). During the six months follow-up, Sensumed Oncologia promoted educational lectures about healthy eating habits and provided guidelines about myths and truths and indications and contraindications of regular physical exercise.
Data regarding age, sex, comorbidities, morbid-family history and life habits were collected by brief anamnesis. Body weight and height were measured for the calculation of BMI, serial laboratory exams were obtained and bioimpedance was performed.
Descriptive analysis of the continuous variables is reported as the mean and as absolute and percent frequency. Data were analyzed statistically using the Excel 2010 software.
RESULTS
Initially, 41 employees satisfied the criteria for inclusion in the project. Of these, 4 did not wish to participate in the Good Life project and one was excluded after becoming pregnant during the study.
Of the 36 employees who started the project, only 29 were submitted to medical examination for the calculation of BMI. However, only 18 subjects fully participated in the first phase of the project and were submitted to bioimpedance, BMI calculation and laboratory tests. These same 18 employees then participated in the second phase of the project with repetition of the exams for comparative analysis (Table 1).
|
Variables |
N |
% |
|
Gender |
||
|
Male |
3 |
16.67% |
|
Female |
15 |
83.33% |
|
Age |
||
|
20-30 years |
8 |
44.44% |
|
31-40 years |
3 |
16.67% |
|
41-50 years |
6 |
33.33% |
|
>50 years |
1 |
5.56% |
|
Morbid-personal history |
||
|
Cardiovascular diseases and/or Diabetes Mellitus |
1 |
5.56% |
|
They deny cardiovascular diseases and/or Diabetes Mellitus |
17 |
94.44% |
|
Morbid-family history |
||
|
Cardiovascular diseasesand/or Diabetes Mellitus |
13 |
72.22% |
|
They deny cardiovascul diseases and/or Diabetes Mellitus |
5 |
27.78% |
|
Alcoholism |
||
|
Yes |
9 |
50.00% |
|
No |
9 |
50.00% |
|
Smoking |
||
|
Yes |
1 |
5.56% |
|
No |
17 |
94.44% |
|
Physical exercise |
||
|
Yes |
13* |
72.22% |
|
No |
5 |
27.78% |
Table 1: Socio-epidemiological characteristics.
Note: *Five of the 13 employees started physical activity after the beginning of the project.
Socio-epidemiological data
The participants responded to an initial questionnaire concerning the following data: gender,age, morbid-personal history, morbid-family history, alcohol consumption, smoking, and physical activity (quantitated as hours/week). The data are presented in table 1.
Among the participants, 83.33% were females and 16.66% were males. Only one participant reported a morbid-personal history of cardiovascular disease and/or diabetes, while 72.22% reported diseases as morbid-family antecedents.
Regarding life habits, 50% of the employees reported social alcohol drinking and only one was a smoker. The practice of physical activity at a frequency of 3 times a week or more was reported by 72.22% of the subjects. Of the 13 employees who engaged in physical activity, 5 started to do so after the beginning of the project.
The mean value of the practice of physical activity among the 13 subjects who engaged in physical activity was 3.55 hours/week, with no marked differences between genders, with 3.5 hours/week among women and 3.6 hours/week among men.
Weight loss
Twenty-nine of the 36 participants attended the weighing sessions on the dayspreviously scheduled (Initial Month and Month 6 of follow-up) and were therefore submitted to BMI calculation for comparative analysis.
Eleven participants coursed with a weight gain ranging from 0.22% to 5.57% of body weight, with a total positive gain of 19.3kg. The remaining 18 employees coursed with a weight loss in the 1.08-14.34% range, for a total loss of 43.74kg, as shown in table 2 and 3.
|
Initial Weight (kg) |
BMI 1 |
Final Weight (kg) |
BMI 2 |
% Variation |
|
(kg/m2) |
(kg/m2) |
|||
|
86 |
31.5 |
86.6 |
31.8 |
0.70% |
|
53.9 |
22.7 |
56.2 |
23.7 |
4.27% |
|
69.15 |
29.1 |
73 |
30.8 |
5.57% |
|
70 |
26.3 |
68.3 |
25.7 |
-2.43% |
|
63.5 |
23.6 |
63.5 |
23.6 |
0.00% |
|
105.8 |
34.9 |
100.8 |
33.3 |
-4.73% |
|
60 |
24 |
58.8 |
23.6 |
-2.00% |
|
61.9 |
25.1 |
61.1 |
24.8 |
-1.29% |
|
62.3 |
25.5 |
63.6 |
25.6 |
2.09% |
|
71.75 |
25.4 |
72 |
25.5 |
0.35% |
|
74.2 |
26 |
70.7 |
24.8 |
-4.72% |
|
58 |
21.3 |
60.1 |
22.1 |
3.62% |
|
46.8 |
16.8 |
45 |
16.1 |
-3.85% |
|
52.3 |
23.6 |
50.6 |
22.8 |
-3.25% |
|
89.8 |
29.3 |
90 |
29.4 |
0.22% |
|
93.2 |
36.9 |
90.1 |
35.6 |
-3.33% |
|
68.84 |
25.9 |
67.6 |
25.5 |
-1.80% |
|
81.6 |
34.4 |
69.9 |
29.5 |
-14.34% |
Table 2: Weight loss (Participated in all stages of the project).
Source: Original elaboration.
BMI: Body Mass Index.
|
Initial Weight (kg) |
BMI 1 |
Final Weight (kg) |
BMI 2 |
% Variation |
|
(kg/m2) |
(kg/m2) |
|||
|
72.9 |
26.7 |
71.6 |
26.3 |
-1.78% |
|
78.9 |
26.4 |
78.1 |
26.1 |
-1.01% |
|
75.8 |
29.6 |
79.8 |
31.2 |
5.28% |
|
74.2 |
28.2 |
73.4 |
28 |
-1.08% |
|
59.6 |
24.4 |
57.8 |
23.8 |
-3.02% |
|
51.1 |
21.8 |
52.1 |
22.3 |
1.96% |
|
93.2 |
36.9 |
90.1 |
35.6 |
-3.33% |
|
68.84 |
25.9 |
67.6 |
25.5 |
-1.80% |
|
81.6 |
34.4 |
69.9 |
29.5 |
-14.34% |
|
83 |
33.2 |
83 |
33.2 |
0.00% |
|
77.9 |
26.3 |
80.3 |
27.1 |
3.08% |
|
101.5 |
33.3 |
96.4 |
31.8 |
-5.02% |
|
68 |
23 |
65.8 |
22.8 |
-3.24% |
|
79.4 |
31 |
80.7 |
31.5 |
1.64% |
Table 3: Weight loss (Only participated in the weighing phase).
Source: Original elaboration.
BMI: Body Mass Index.
Laboratory exams
The results of the laboratory exams are reported as sample mean and percent variation. After 6 months of health-promoting activities, 61.11% of the participants showed a reduction of glycemia levels compared to the sample obtained in the first month, and basal insulin was reduced in 55.56% of the study sample. HDL cholesterol increased in only 16.67% of cases, but LDL levels decreased in 61.11% of cases.
It should, also, be pointed out that there was an important change in triglyceride levels, with 94.44% of the participants showing a reduction of basal rates.
Cholesterol variation: On the occasion of the first blood collection for laboratory exams, the mean total cholesterol value was 178.2mg/dL for women and 207.6mg/dL for men, LDL cholesterol was 102.2mg/dL for women and140.6mg/dL for men, and HDL cholesterol HDL was 55.8mg/dL for women and 45.3mg/dL for men.
In the second sample obtained in the 6th month of follow-up, total cholesterol amd LDL cholesterol levels were reduced in both men and women, but there was also a reduction of HDL cholesterol. The mean total cholesterol value was 129.8mg/dL for women and 206.6mg/dL for men and the nean LDL cholesterol value was 87.0mg/dL for women and 149mg/dL for men. However, the mean HDL cholesterol value was reduced to 38.8mg/dL for women and 38.3mg/dL for men, as shown in figure 1.
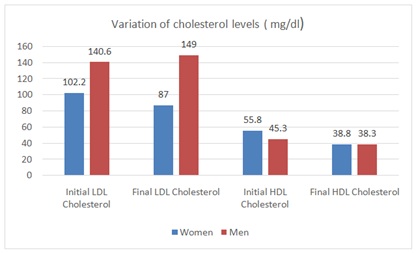 Figure 1: Cholesterol level in the 2nd laboratory test sample.
Figure 1: Cholesterol level in the 2nd laboratory test sample.
Triglyceride variation:
An important reduction in triglyceride rates occurred during the study, especially among women, as shown in figure 2. The mean triglyceride value was reduced from 101.9mg/dL in the first sample to 55.26mg/dL in the second for women and from 106.6mg/dL to 98.6mg/dL for men.
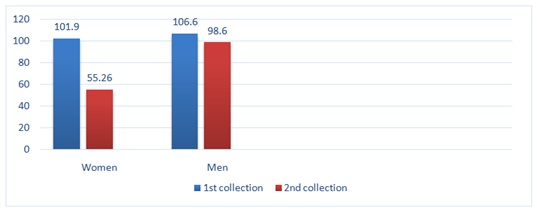 Figure 2: Variation of triglycerides between the 1st and 2nd sample for laboratory tests.
Figure 2: Variation of triglycerides between the 1st and 2nd sample for laboratory tests.
Variation of glycemia and basal insulin: Mean fasting glycemia was 74.6mg/dL in the first exam and 72.6mg/dL in the second for women, as shown in table 4, and basal insulin was reduced from 7mcU/mL to 5.9mcU/mL. For men, mean glycemia was 77mg/dLin the first exam and was reduced to 70mg/dLin the second; Among men, basal insulin increased from 5.7mcU/mL to 6.5mcU/mL, as shown in table 5.
|
Mean for Women |
Mean for Men |
|
|
Glycemia initial month |
74.6mg/dl |
77mg/dl |
|
Glycemia month 6 |
72.6mg/dl |
70mg/dl |
Table 4: Variation of mean fasting glycemia values.
|
Variable |
Mean for Women |
Mean for Men |
|
Insulininitial month |
7.0mcu/ml |
5.7mcu/ml |
|
Insulinmonth 6 |
5.9mcu/ml |
6.5mcu/ml |
Table 5: Variation of mean basal insulin values.
Bioimpedance: The mean variation of bioimpedance from the first to the sixth month was not so expressive. Lean mass increased from 66.3 to 67.4% among women and decreased from 75.9 to 75.8% among men, as shown in figure 3.
 Figure 3: Variation of mean bioimpedance values in the 1st and 6th month (lean mass).
Figure 3: Variation of mean bioimpedance values in the 1st and 6th month (lean mass).
DISCUSSION
Obesity is a major public health problem, being related to cardiovascular, metabolic, oncologic, mental, psychological and social health. The calamity for the health of both developed and developing countries is that obesity is starting and becoming established at increasingly earlier ages [1,13,14].
The prevalence of overweight (BMI>25kg/m2) and of obesity (BMI>30kg/m2) is progressively increasing, a reality that is also being observed in the city of Manaus. The cause of obesity is known to be multifactorial, although the major features of the disease are due to the increased intake of industrialized food, to a reduction of energy expenditure by the population and to the lack of physical activity in the daily routine [15].
Published investigations have demonstrated that the encouragement of changes in community life style can have positive results, in addition to interventions in health promotion and in the habits of people. The promise study conducted in England has shown important positive weight loss in primary care when coaches and health agents specializing in the promotion of physical activity and in patient follow-up provide support measures [16-18].
Another study measured social support for a healthy diet and the practice of physical activity for 12 months in a weight loss program. The results suggested that solid psychometric measures can be used for knowledge and for personalized clinical interventions with the social support of relatives or of close friends who co-participate in the challenge of weight loss [19].
The Good Life project showed that even though most employees did not have a diagnosis of cardiovascular or metabolic comorbidities, they had a family history of these conditions that placed them at risk depending on the lifestyle they adopted. Another interesting results was the initiation of regular physical activity at a frequency of 3 times a week or more, which caused five of the 18 employees (27.7%) to leave behind their sedentary status.
During the six months of the project, dynamic interactive lectures were offered to the participants about health promotion, contemplating the main modifiers of obesity, i.e., a healthy diet and regular physical exercise, as well as reinforcement of good habits for quality of life, with discouragement of practices such as smoking, alcohol drinking and sedentarism.
Another important aspect of weight loss is its impact on the quality of life of people. Several studies have demonstrated that, psychologically, excess weight is directly associatedwith low self-esteem, a negative self-image and social stigmatization and discrimination. Validated questionnaires have demonstrated a significant improvement of subjects participating in weight loss programs after 6 months [14,18,20].
Due to the previously mentioned risks of excess weight, several measures are being applied in order to reduce, prevent or treat obesity, such as non-pharmacological treatment with changes in lifestyle and pharmacological or surgical treatment [21].
Among the main non-pharmacological measures is the introduction of regular physical activity and a healthy diet, even though the adoption of simple tasks such as the reduction of sitting time during the daily routineand an increased frequency of movement can have an impact on the reduction or maintenance (another great challenge) of ideal weight [21].
Analysis of the 29 employees who were weighed both at the beginning and at the end of the project showed a total loss of 43.74kg. Weight loss is directly related to a better control and, in some cases, to the complete resolution of comorbidities such as sleep apnea, diabetes mellitus and hypertension, as reported in a study on the evolution of quality of life and loss of comorbidities in patients submitted to bariatric surgery [14].
Creating an environment that favors good health practices in the workplace, where most of the population spends most of its functional time of day, can generate positive results regarding quality of life and health. The methods described are of low cost and of easy application when compared to pharmacological treatment and surgical intervention.
Regarding the laboratory exams, we observed that the parameters mostly impacted by weight loss were those related to the lipid profile (total cholesterol, LDL cholesterol and triglycerides), although the basal levels of HDL cholesterol were slightly reduced despite the increase in physical activity among the participants. It is important to point out that no questionnaire about diet control was applied to the participants, so that it was not possible to relate HDL cholesterol levels to the diet adopted.
However, a study with nutritional intervention conducted over a period of 4 months demonstrated a significant reduction of BMI, abdominal circumference, glycemia and triglycerides after changes in eating habits, although without evidence of important improvement of HDL or LDL cholesterol, in agreement with the results of the present study [22].
The bioimpedance exams performed in the initial month and in the 6th month of follow-up in the 18 participants who concluded all the stages of the project showed a discrete increase in lean mass gain among women and a smaller variation in lean mass among men, who had a slightly more modest reduction.
A study reporting intervention with regular physical activity over a period of 4 months showed reduction of systolic pressure, cardiorespiratory conditioning, flexibility and improvement of the metabolic profile and glycemia in a group of hypertensive persons. However, it was observed that during the study period it was not possible to reduce fat percent or BMI in a significant manner, as also observed in the present study [23].
The Good Life project had some limitations. The employees of the company worked in two shifts, a fact that impaired the execution of certain steps of the project by some participants, such as the application of laboratory tests to subjects who only worked in the afternoon shift. Another limitation was the lack of detailed control of adhesion to the diet and physical activity during the study period. Also, psychological or emotional aspects were not evaluated. Finally, the observational design of the study did not permit direct interventions in the life habits of the study population.
AUTHORS’ CONTRIBUTIONS
Ananda Castro Chaves, Abner Souza Paz, Ana Cecília de Souza Lima, Rafaela Melo Campos Borges, and Caroline Souza dos Anjos conceived the study and interpreted the data. Caroline Souza dos Anjos and Lia Mizobe Ono performed a critical revision. Caroline Souza dos Anjos and William Hiromi Fuzita approved the final vesion of the paper.
CONFLICTS OF INTEREST
None.
ACKNOWLEDGMENT
We are grateful to Sensumed Oncologia for support with the conception and development of the project.
REFERENCES
- ABESO (2016) Diretrizes Brasileiras de Obesidade. Associação Brasileira para o Estudo da Obesidade e da Síndrome Metabólica, São Paulo, Brazil.
- Nunes RR, Clemente ELS, Pandini JÁ, Cobas RA, Dias VM, et al. (2009) Confiabilidade da classificação do estado nutricional obtida através do BMI e três diferentes métodos de percentual de gordura corporal em pacientes com diabetes melito tipo 1. Arq Bras Endocrinol Metabol 53: 360-367.
- Douketis JD, Macie C, Thabane L, Williamson DF (2005) Systematic review of long-term weight loss studies in obese adults: Clinical significance and applicability to clinical practice. Int J Obes (Lond) 29: 1153-1167.
- Colditz GA, Sellers TA, Trapido E (2006) Epidemiology-identifying the causes and preventability of cancer? Nat Rev Cancer 6: 75-83.
- Knowler WC, Barrett-Connor E, Fowler SE, Hamman RF, Lachin JM, et al. (2002) Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N Engl J Med 346: 393-403.
- Prado WL, Siegfried A, Dâmaso AR, Carnier J, Piano A, et al. (2009) Effects of long-term multidisciplinary inpatient therapy on body composition of severely obese adolescents. J Pediatr (Rio J) 85: 243-248.
- Diretrizes da Sociedade Brasileira de Diabetes 2017-2018/Organização José Egídio Paulo de Oliveira, Renan Magalhães Montenegro Junior, Sérgio -- São Paulo: Editora Clannad, 2017.
- Instituto Nacional do Cân Peso Corporal.
- Simão AF, Precoma DB, Andrade JP, Correa Filho H, Saraiva JFK, et al. (2013) I Diretriz Brasileira de Prevenção Sociedade Brasileira de Cardiologia (6, Supl. 2).
- Franzoni B, Lima LA, Castoldi L, Labrêa MGA (2013) Avaliação da efetividade na mudança de hábitos com intervenção nutricional em grupo. Cien Saude Colet 18: 3751-3758.
- Machado JC, Cotta RMM, Silva LS (2014) Abordagem do desvio positivo para a mudança de comportamento alimentar: Revisão sistemáti Rev Panam Salud Publica 36: 134-140.
- Viana LV, Paula TP, Leitão CB, Azevedo MJ (2013) Fatores determinantes de perda de peso em adultos submetidos a intervenções dietoteráp Arq Bras Endocrinol Metabol 57: 717-721.
- McDowell K, Petrie MC, Raihan NA, Logue J (2018) Effects of intentional weight loss in patients with obesity and heart failure: A systematic review. Obes Rev 19: 1189-1204.
- Castanha CR, Ferraz AAB, Castanha AR, Belo GQMB, Lacerda RMR, et al. (2018) Avaliação da qualidade de vida, perda de peso e comorbidades de pacientes submetidos à cirurgia bariátrica. Rev Col Bras Cir 45: 1864.
- Malta DC, Andrade SC, Claro RM, Bernal RTI, Monteiro CA (2014) Evolução anual da prevalência de excesso de peso e obesidade em adultos nas capitais dos 26 estados brasileiros e no Distrito Federal entre 2006 e 2012. Rev Bras Epidemiol Suppl Pense 17: 267-276.
- Dutton GR, Lewis CE, Cherrington A, Pisu M, Richman J, et al. (2018) A weight loss intervention delivered by peer coaches in primary care: Rationale and study design of the PROMISE trial. Contemp Clin Trials 72: 53-61.
- Nor NSM, Ambak R, Aris T (2018) An introduction to the my body is fit and fabulous at home (MyBFF@home): A community-based weight loss intervention study among Malaysian housewives. BMC Womens Health 18: 107.
- Perez-Sousa MA, Olivares PR, Escobar-Alvarez JA, Parraça JA, Gusi N (2018) Fitness as mediator between weight status and dimensions of health-related quality of life. Health and Qual Life Outcomes 16: 155.
- Rieger E, Sellbom M, Murray K, Caterson I (2018) Measuring social support for healthy eating and physical activity in obesity. Br J Health Psychol 23: 1021-1039.
- Ambak R, Nor NSM, Puteh N, Tamil AM, Omar MA, et al. (2018) The effect of weight loss intervention programme on health-related quality of life among low income overweight and obese housewives in the MyBFF@home study. BMC Women's Health 18: 111.
- Fanning J, Opina MT, Leng I, Lyles MF, Nicklas BJ, et al. (2018) Empowered with Movement to Prevent Obesity & Weight Regain (EMPOWER): Design and methods. Contemp Clin Trials 72: 35-42.
- Busnello FM, Bodanese LC, Pellanda LC, Santos ZEA (2011) Intervenção nutricional e o impacto na adesão ao tratamento em pacientes com síndrome metabóli Arq Bras Cardiol 97: 217-224.
- Monteiro HL, Rolim LMC, Squinca DA, Silva FC, Ticianeli CCC, et al. (2007) Efetividade de um programa de exercícios no condicionamento físico, perfil metabólico e pressão arterial de pacientes hipertensos. Rev Bras Med Esporte 13: 107-112.
Citation: Chaves AC, Borges RMC, Lima AC, Paz AS, Ono LM, et al. (2019) Good Life Project: Description of the Impact of Weight Loss Intervention at a Private Health Service in Manaus. J Food Sci Nut 5: 046.
Copyright: © 2019 Ananda Castro Chaves, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.