Inequalities in the Women’s Empowerment and their Vulnerability to HIV in India
*Corresponding Author(s):
Ana CatShri Kant SinghDepartment Of Mathematical Demography And Statistics, International Institute For Population Sciences, Mumbai, India
Tel:+91 9869229110,
Email:sksingh31962@gmail.com
Abstract
Background and objectives: Over the years, there has been growing evidence of continuous narrowing gender gap in new HIV infections, despite stagnation in the overall prevalence of HIV in India. Among others, one of the reasons behind the existing pattern in HIV/AIDS in the country is the poor status of women, lack of control over sexuality and poor reproductive and sexual rights among women. NFHS-4 results portray profound increase in woman’s status and empowerment in India in the recent years. Therefore, this paper aims to analyze the relationship between woman’s empowerment, their HIV vulnerability and prevalence of HIV across different states in India.
Data and methods: This paper utilizes the data from two rounds of National Family Health Surveys, Indian version of Demographic and Health Surveys (DHS) conducted in 2005-06 (NFHS-3) and 2015-16 (NFHS-4) respectively and information collected through National Sentinel Surveillance conducted by National AIDS Control Programme during 2012-2015.
Results: Despite the increase in women empowerment in the recent years, the comprehensive knowledge of HIV/AIDS, a means to reduce women’s vulnerability to HIV/AIDS, has not improved significantly. The level of spousal violence has reduced by almost 20 percent in the last one decade (2005-2015) and women participation in household decision making has also increased significantly across different states. Further, there is an extensive awareness among women regarding condom use as a protection against HIV. However, the recent evidence from NFHS 4 and Sentinel Surveillance do not support pronounced association between women’s empowerment and consistent condom use visa V is prevalence of HIV, which has been evident in most of sub Saharan African Countries. The relationship seems to be spurious, especially in well-known high HIV prevalence states of India like Andhra Pradesh, Maharashtra, Manipur and Karnataka.
Conclusions: All programs to curve the pace of HIV epidemic focusing at reducing woman’s vulnerability to HIV/AIDS, should not merely focus at general woman’s empowerment but there should be specific awareness and capacity building programmes addressing comprehensive knowledge and condom promotion among women.
Keywords
INTRODUCTION
WOMEN AND HIV PANDEMIC
Women are relatively more vulnerable to HIV as they are not only detached from socio-economic opportunities but are denied of access to health care services in many parts of the country [5]. The vulnerability of women can be attributed to a socio-economic and cultural context of India. Women are always susceptible and, therefore, lack awareness in various fields including access and utilization of health care services [5], which has resulted in the growth of women suffering from STI/HIV. According to HIV estimations India [6], HIV prevalence among national adult (15-49 years) is estimated at 0.26% (0.22%-0.32%) in 2015. Further, the prevalence of HIV in 2015 among males is estimated at 0.30% and among females is estimated at 0.22% in comparison to 2007 which estimated 0.40 among males and 0.26 among females. This confirms a clear decline in the prevalence of HIV nationally but there is narrowing gender gap in the overall prevalence as well as in new HIV diagnosis, which means that the gap of decline in HIV prevalence is less among females comparatively. Data also reveals that women continue to account for more than 40% of people living with HIV infection in the country [6].
POVERTY AND HIV
FMH can occur as an acute or chronic event. In the chronic presentation, the hemorrhage has been prolonged or repeated during pregnancy, anemia developed slowly, giving the fetus the opportunity to develop hemodynamic compensation. In this case, the diagnosis is often postnatal and these infants may manifest only pallor at birth with no other complications [5].
In opposition, in acute FMH, perinatal hypoxia and intrauterine death or severe anemia and hypoxia at birth can be present [5].
Neonatal anemia was the first manifestation of FMH in 35% of the reported cases. In severe ones, shock and circulatory failure may be present [6].
In our clinical report, it’s more likely to be a chronic transfusion given the rapid ability of the newborn to adapt to extra uterine life despite the hemoglobin value at birth. The absence of fetal movements noted by the mother was not due to the FMH but it was caused by the circular of the umbilical cord around the arms that made it impossible to the fetus to move.
Abdominal trauma and invasive techniques of prenatal diagnosis are related to FMH [1]. Physicians should consider alternative diagnosis to neonatal anemia such as isoimmune hemolytic anemia, congenital infections that result in bone marrow suppression (TORCH), sepsis, congenital erythrocyte defects and congenital hemoglobinopathies [6]. Clinical and laboratory evaluation of infection, Coombs test and viral serology should be performed.
In this case, the diagnosis of FMH was confirmed by the KB test. Pink fetal red blood cells are observed and counted in the mother’s peripheral blood smear because fetal hemoglobin is resistant to acid elution, leaving discolored maternal cells (patients with sickle cell anemia or hereditary persistence of fetal hemoglobin may lead to a false positive result and ABO incompatibility may produce a false negative result) [2].
Although the KB test is inexpensive and requires no special equipment, it lacks standardization and is imprecise [3]. Flow cytometry, based on the use of anti-fetal hemoglobin for detection of fetal cells with fetal hemoglobin, represents an improvement of KB test since is more specific and precise [7].
Although the prognosis of massive FMH is poor, it can be improved if physicians early recognize this condition. When the infant is near-term gestation, immediate cesarean delivery is indicated. If, on the other hand, the fetus is still preterm, in uterus transfusion can be considered and has been shown to be effective and improves the prognosis [6].
Long term outcome for infants affected by massive FMH is unfavorable with death or neurological dysfunction [6]. The prognosis is more directly related to initial hemoglobin value and clinical manifestations post-delivery than with the transfused volume of blood [8].
The case reported emerged from a pregnancy with no risk factors. Mother’s perception of decreased fetal movements, recognition of fetal distress on the CTG, immediate caesarean section and prompt hemodynamic and respiratory support to the newborn with early red blood cells transfusion contributed for this good outcome.
AUTONOMY AND HIV
DATA AND METHODOLOGY
Women’s vulnerability to HIV has been assessed through comprehensive knowledge, which describes having correct knowledge of HIV prevention and also rejects two most common misconceptions. These knowledge includes having knowledge that consistent use of condom and having just one uninfected partner limit the risk of getting AIDS, knowledge that a healthy looking person can also have AIDS and rejecting the two most common misconceptions about AIDS transmission (transmission by mosquito bites and by sharing food).The comprehensive knowledge has been taken as a dependent variable to assess the vulnerability in terms of inequality among women.
The inequality in women’s empowerment is computed by using Lieberson’s Diversity Index. This index defines the homogeneity and heterogeneity of spatial inequality across different states in India. The index is defined as follows:
If Ci (i=1,2,3,….n) denotes the proportion of individuals in the ith subclass such that ∑Ci = 1, then Lieberson’s index of Diversity (D) is defined as
D= 1-∑ni = 1Ci2
Theoretically the diversity index varies from 0 to 1. Zero in case of perfect homogeneity when the inequality is almost nil and one in case of perfect heterogeneity, a case where there is maximum inequality.
RESULTS
Women’s empowerment
Table 1 presents the percentage of women owning different household assets namely ownership of house/land, having a bank/saving account and owning a mobile phone. In the context of ownership of house/land by women, Manipur seizes the highest rank (70%) followed by Bihar (59%), Meghalaya (57%) and Tripura (57%). Similarly, little more than half of women in Karnataka (52%) and half women in Telangana (50%) own house/land in their name alone or jointly with other family members. On the other hand, less than half of women in Maharashtra and one-fourth of women in West Bengal and one-fourth of women in Sikkim own a house/land. In case of women having a bank account, more than 80 percent women in Goa and Andaman and Nicobar Islands have their own bank/saving account followed by women in Tamil Nadu (77%), Puducherry (68%), Andhra Pradesh (64%) and Sikkim (60%). Further, around 50-60 percent of women in Telangana, Karnataka, Tripura and Uttarakhand reported having their own bank/saving account. On the other hand, only a little more than two-fifths of women in Maharashtra and only one-fourth of women in Bihar have their own bank/savings account. In case of ownership of mobile phone, it was found that more than one-fourth of women in all the states and union territories own a mobile phone, which they can use on their own. More than 80 percent of women in Goa and Sikkim followed by a little less than three-fourths of women in both Andaman and Nicobar Island and Puducherry own mobile phone. Madhya Pradesh is the only state where less than 30% of women own a mobile phone.
| State/UTs | Owning House or Land | Bank Account | Mobile |
| Andaman & Nicobar Islands | 29.7 | 81.8 | 66.9 |
| Andhra Pradesh | 44.7 | 66.3 | 36.2 |
| Bihar | 58.8 | 26.4 | 40.9 |
| Goa | 33.9 | 82.8 | 80.9 |
| Haryana | 35.8 | 45.6 | 50.5 |
| Karnataka | 51.8 | 59.4 | 47.1 |
| Meghalaya | 57.3 | 54.4 | 64.3 |
| Madhya Pradesh | 43.5 | 37.3 | 28.7 |
| Maharashtra | 34.3 | 45.3 | 45.6 |
| Manipur | 68.9 | 34.8 | 63.1 |
| Puducherry | 40.3 | 68.2 | 67.3 |
| Sikkim | 24.8 | 63.5 | 79.8 |
| Telangana | 50.5 | 59.7 | 47.8 |
| Tamil Nadu | 36.2 | 77 | 62 |
| Tripura | 57.3 | 59.2 | 43.9 |
| Uttarakhand | 29.2 | 58.5 | 55.4 |
| West Bengal | 23.8 | 43.5 | 41.9 |
Spousal violence is a problem that is entrenched in many societies around the world and India is no exception. Although societal awareness and condemnation of the issue have increased in recent years, spousal violence remains a hidden and persistent problem because of the power and control held by the abuse and humiliation suffered by the victims of this crime [15]. Figure 1 portrays a comparative proportion of ever married women experiencing spousal violence in NFHS-3 to NFHS-4. The data reveals that there has been a decline in overall spousal violence in most of the states except for Haryana, Manipur and Meghalaya. Among all the states, the highest decline (around 16%) in proportion of women experiencing spousal violence is found in Sikkim, Tripura and Bihar. Similarly, the decline in spousal violence of ever-married women is found in states like Uttarakhand by 15 percent, Madhya Pradesh by 12 percent and Maharashtra and West Bengal by less than 10 percent .In contrary, the women experiencing spousal violence has increased by 16 percent in Meghalaya followed by 9 percent in Manipur and 5 percent in Haryana. Though the prevalence is still high but it shows a declining trend in most of the states.
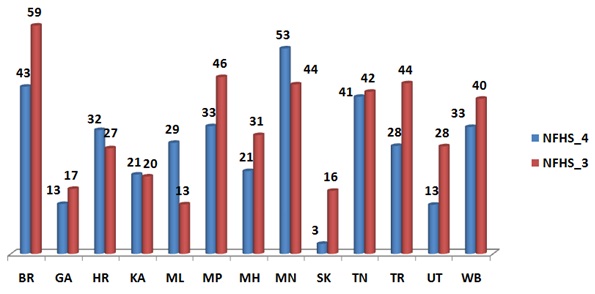
Figure 1: Percentage of ever married women who have ever experienced spousal violence (NFHS-3 to NFHS-4).
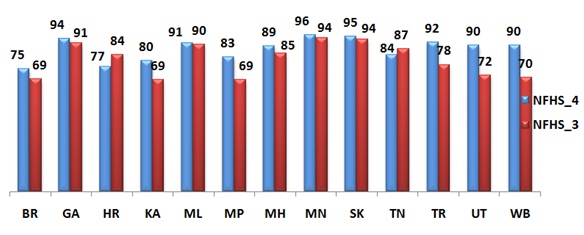
One of the important indicators in measuring empowerment of women is the autonomy of women in decision making both in social and household life [16]. Figure 2 represents the change from NFHS-3 to NFHS-4 in the proportion of women who reported to participate in household decision making. Results reveal that in totality there has been an increase in the participation level at household level by more than three-fourths of women in all the states, except for the state of Haryana and Tamil Nadu. In these two states the participation level at household is found decreasing by 7 and 3 percent point respectively. The proportion of women participating in household level decision making has crossed over 90 percent in states like Sikkim, Goa, Meghalaya, Manipur and Tripura. This shows that these states have a very conducive environment to exercise their reproductive and sexual rights, which may reduce their HIV vulnerability.
HIV vulnerability
The most recent evidence on data pertaining to proportion of women having comprehensive knowledge of HIV/AIDS portrays that there is not much improvement in the level of comprehensive knowledge level of HIV/AIDS among adult women age 15-49 in the last one decade i.e., from NFHS-3 to NFHS-4. It is evident from table 2 that less than 30 percent of the women have comprehensive knowledge of HIV/AIDS in states and union territories like Andhra Pradesh, Puducherry, Telangana and Andaman and Nicobar Islands in NFHS-4. Though there has been increase in comprehensive knowledge of HIV/AIDS in Tripura by 10-19 percent point but in some states like Goa, Haryana, Meghalaya, Sikkim, Tamil Nadu, Maharashtra and West Bengal, it has increased only by less than 10 percent point. Further, the comprehensive knowledge of HIV/AIDS among women in states like Bihar, Karnataka, Madhya Pradesh, Manipur and Uttarakhand is seen decreasing, which limits the country to reach the Millennium Development Goals despite increasing women’s status and empowerment.
| State/UTs | Women who have knowledge of consistent condom use | Women who have knowledge of consistent condom use | ||
| NFHS_4 | NFHS_3 | NFHS_4 | NFHS_3 | |
| Andaman & Nicobar Islands | 29.3 | N.A | 59.5 | N.A |
| Andhra Pradesh | 29.0 | N.A | 57.5 | N.A |
| Bihar | 10.1 | 11.7 | 33.5 | 22.8 |
| Goa | 34.6 | 28.5 | 77.4 | 47.6 |
| Haryana | 31.1 | 24.7 | 71.6 | 46.0 |
| Karnataka | 9.5 | 11.6 | 50.0 | 34.8 |
| Meghalaya | 13.3 | 13.1 | 47.0 | 26.2 |
| Madhya Pradesh | 18.1 | 20.3 | 46.8 | 37.8 |
| Maharashtra | 25.4 | N.A | 72.7 | N.A |
| Manipur | 25.5 | 22.2 | 62.7 | 56.5 |
| Puducherry | 29.5 | N.A | 59.0 | N.A |
| Sikkim | 16.0 | 12.3 | 64.7 | 41.9 |
| Telangana | 28.0 | 11.8 | 57.6 | 41.7 |
| Tamil Nadu | 28.6 | 28.7 | 65.3 | 54.7 |
| Tripura | 18.6 | 9.8 | 53.9 | 30.4 |
| Uttarakhand | 30.0 | 29.5 | 67.9 | 46.9 |
| West Bengal | 40.7 | 44.0 | 79.0 | 79.1 |
There are a number of factors - Biological, Socio-cultural and Economic which make women more vulnerable to HIV/AIDS. Syndemic risk (which is a function of violence, substance use, perceived financial hardship, emotional distress and self-worth) affects women with and at risk for HIV [20]. Women are twice as likely as men to contract HIV from a single act of unprotected sex [14]. Condom use is a critical element in a comprehensive, effective and sustainable approach to HIV prevention and treatment [21]. Women can play a vital role in the prevention of HIV as it will not only help them in protecting themselves but also their children against it [11]. Therefore, it is important to assess the awareness or knowledge of women regarding consistent condom use as a protection of HIV/AIDS. Last two columns of table 2 represent the change in proportion of women having knowledge that consistent condom use as protection against HIV in NFHS-3 to NFHS-4. The data shows that overall in all the states there is an increasing trend in the awareness level of women regarding condom use as protection against HIV. In some of the states like Goa, Maharashtra and West Bengal, there has been an increase in the awareness level by more than 20% point followed by an increase in awareness level of women in Meghalaya and Tripura by 10-19% point. Whereas in states like Bihar, Haryana, Madhya Pradesh, Sikkim, Manipur and Uttarakhand there has been an increase in the awareness level by less than 10% point among women regarding the knowledge that consistent condom use is a protection against HIV.
Inequality and HIV vulnerabilities
| State/UT | Comprehensive Knowledge | Owning House or Land | Bank Saving Account | Mobile Phone | Spousal Violence | Household Decision Making |
| Andaman & Nicobar Islands | 29.3 | 0.616 | 0.659 | 0.659 | 0.642 | 0.657 |
| Andhra Pradesh | 29.0 | 0.921 | 0.922 | 0.922 | 0.908 | 0.920 |
| Bihar | 10.1 | 0.972 | 0.969 | 0.972 | 0.969 | 0.971 |
| Goa | 34.6 | 0.377 | 0.499 | 0.497 | 0.496 | 0.495 |
| Haryana | 31.1 | 0.946 | 0.948 | 0.952 | 0.94 | 0.950 |
| Karnataka | 9.5 | 0.964 | 0.965 | 0.962 | 0.96 | 0.963 |
| Meghalaya | 13.3 | 0.822 | 0.840 | 0.835 | 0.694 | 0.842 |
| Madhya Pradesh | 18.1 | 0.976 | 0.975 | 0.973 | 0.976 | 0.975 |
| Maharashtra | 30.0 | 0.967 | 0.969 | 0.969 | 0.961 | 0.970 |
| Manipur | 40.7 | 0.877 | 0.867 | 0.866 | 0.903 | 0.865 |
| Puducherry | 25.4 | 0.706 | 0.748 | 0.742 | 0.663 | 0.738 |
| Sikkim | 25.5 | 0.649 | 0.660 | 0.670 | 0.625 | 0.672 |
| Tamil Nadu | 16.0 | 0.964 | 0.968 | 0.968 | 0.971 | 0.967 |
| Tripura | 28.0 | 0.697 | 0.692 | 0.660 | 0.749 | 0.697 |
| Uttarakhand | 28.6 | 0.904 | 0.916 | 0.915 | 0.864 | 0.911 |
| West Bengal | 18.6 | 0.936 | 0.945 | 0.944 | 0.941 | 0.946 |
A combined effect of all these variables on comprehensive knowledge on HIV/AIDS has also been examined through a multiple linear regression equation that is given below, specifying non-significant relation between different dimensions of woman’s inequalities (X1 to X5) and their HIV vulnerability measured in terms of comprehensive knowledge of HIV(Y);
Y= 89.1+200.0X1+ 296.1X2+399.3X3+76.9X4-1042.5X5
Though the value of unadjusted R square comes to be 44 percent but the value of adjusted R square is 13.4 percent with standard error of 8.6. This shows that there is no significant relationship between women empowerment and comprehensive knowledge of HIV/AIDS. That means women empowerment is not significantly affecting the vulnerability of women in terms of comprehensive knowledge of HIV/AIDS in most of Indian states.
Changing HIV scenario in India
According to UNAIDS report India has the third largest HIV epidemic in the world [22]. Though the prevalence of HIV is lowering in compared to other middle-income countries but because of the large population in India, the prevalence equates to a huge number. Table 4 presents the trend in the percentage of HIV prevalence among adults aged 15-49 years in different states from 2012 to 2015. The trend of HIV prevalence is found decreasing in almost all the states except for Sikkim and Tripura. Apart from that the prevalence of HIV in the states like Haryana, Meghalaya and Uttarakhand has remained constant all these years. In Karnataka, the HIV prevalence is reduced by 0.6% followed by Goa where HIV prevalence is reduced by 0.5% point. In other states like Bihar, Tamil Nadu and West Bengal the reduction in HIV prevalence from 2012 to 2015 is by 0.2% point and in Madhya Pradesh it is just reduced by 0.1% in four-year time span. The overall scenario shows that the country is showing a success in responding to HIV epidemic.
| State/UT | 2012 | 2013 | 2014 | 2015 |
| Andaman & Nicobar Island | 0.08 | 0.08 | 0.07 | 0.07 |
| Andhra Pradesh | 0.74 | 0.71 | 0.68 | 0.66 |
| Bihar | 0.27 | 0.26 | 0.26 | 0.25 |
| Goa | 0.45 | 0.43 | 0.41 | 0.40 |
| Haryana | 0.13 | 0.13 | 0.13 | 0.13 |
| Karnataka | 0.51 | 0.49 | 0.47 | 0.45 |
| Meghalaya | 0.06 | 0.06 | 0.06 | 0.06 |
| Madhya Pradesh | 0.10 | 0.10 | 0.10 | 0.09 |
| Maharashtra | 0.42 | 0.40 | 0.39 | 0.37 |
| Manipur | 1.45 | 1.34 | 1.24 | 1.15 |
| Sikkim | 0.17 | 0.19 | 0.21 | 0.23 |
| Tamil Nadu | 0.30 | 0.30 | 0.29 | 0.28 |
| Tripura | 0.24 | 0.26 | 0.28 | 0.31 |
| Uttarakhand | 0.11 | 0.11 | 0.11 | 0.11 |
| West Bengal | 0.23 | 0.22 | 0.21 | 0.21 |
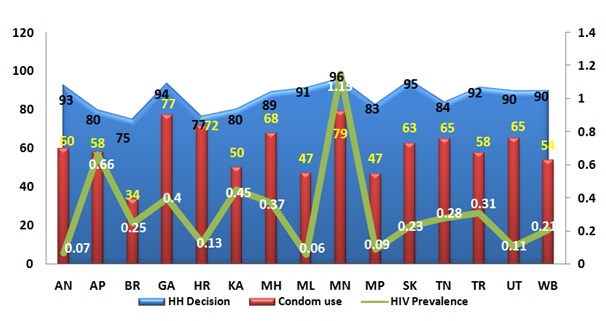
The overlapping graph reflects the women’s autonomy in household decision making and knowledge about consistent condom use, which may be treated as protective factors against their HIV vulnerability among adult women age 15-49 in 15 states of India. Further, it also shows the trend of HIV prevalence in these states as per the recently completed Integrated Biological and Behavioural Survey (2014-15). Figure 3 portrays a contentious relationship between women’s autonomy in decision making, awareness to consistent condom use and the prevalence of HIV. There is high level of women’s autonomy in household decision making and awareness of consistent condom use as a protection against HIV in states like Haryana and Uttarakhand along with the Andaman and Nicobar Island, which has a negative association with the prevalence of HIV. On the other hand, it is surprising to know that the prevalence of HIV is very high in states like Andhra Pradesh, Maharashtra, Manipur and Karnataka despite women’s high level of autonomy in decision making and high awareness regarding consistent condom use as a protection against HIV. But unpredictably in other larger states like Madhya Pradesh, Bihar and West Bengal, the prevalence of HIV maintains to be very low (between 0.09 to 0.25%) despite low level of awareness regarding consistent condom use as a protection against HIV (between 34 to 54%).
DISCUSSION
Women’s vulnerability to HIV/AIDS may be higher among women from states like Sikkim, Goa and West Bengal, where women’s autonomy in decision making has improved considerably but the knowledge about consistent condom use as protection from HIV infection is still low. Similarly, women from Bihar and Meghalaya also lack awareness regarding HIV and its protection despite of high ownership of household assets. The probable reasons might be women are provided with autonomy and technology to some extent but the use of technology for awareness purpose is low. The study by Amin (2003) depicts that awareness messages in India mostly remain neutral in addressing the negative gender and sexual norms fuelling the epidemic. He further argues that most awareness programs scarcely address their risk and need for prevention information. He supports his argument with the following example: Awareness campaigns mainly target high-risk groups to promote and emphasize condom use when practicing high-risk behaviour, but rarely insist that these groups use condom with their wives who remain “uninformed, unaware and unprotected” [16].
Our finding that regardless of decreasing HIV estimates in India, states like Andhra Pradesh, Maharashtra, Manipur and Karnataka are still suffering from high HIV prevalence has also been found in other studies. A recent study by Indian Health Action Trust in 2010, reported that the prevalence of HIV in Maharashtra is high among MSM [25]. So, in Maharashtra the reason for high prevalence might be that HIV exists among MSM (Male having Sex with Male) where female have no role to play. Further, Gregory Armstrong in his study of injecting drug users in North-East [26] found that youth below age of 25 in Manipur is vigorously injecting drugs in their body which might be the cause of high HIV prevalence. The reason for high prevalence of HIV in Andhra Pradesh and Karnataka might be because of unemployment, migration, poor health and unhealthy sexual practices.
Though India has successfully shown progress in halting and reverting the HIV epidemic by expanding treatment, care and support services yet in some states HIV prevalence has been found increasing [6]. As per the report of HIV estimates in India, 2015 it is obvious that the overall trend in HIV prevalence is decreasing but in an account of gender, the prevalence is still high among women. This gives light to the point that there is a lack of comprehensive knowledge about HIV/AIDS and its protection among women especially which is increasing their vulnerability towards HIV.
CONCLUSION AND RECOMMENDATIONS
REFERENCES
- Annan K (2005) Empowering women the most effective development tool. UN News Center, New York, USA.
- Chamar V (2015) Short Essay on Gender Inequality. Social Issues in India, Important India, India.
- Mondal P (2015) Essay on Women Empowerment in India. Young Article Library, 31317.
- Raju S, Jatrana S (2016) Women workers in Urban India, Cambridge University Press, New Delhi, India.
- Chatterjee P (1999) The Nation and its Women. In: Chatterjee P, Partha Chatterjee Omnibus, OUP India.
- NACO, NIMS (2015) India HIV Estimations: Technical Report. Ministry of Health & Family Welfare Government of India, India.
- Hess C, Roman S (2016) Poverty, Gender, and Public Policies. Institute for Women’s Policy Research, Washington, DC, USA.
- van Donk M, Msiska R (2002) Conceptual shifts for sound planning: towards an integrated approach to HIV/AIDS and poverty. UNDP, Pretoria, South Africa.
- The World Bank (1997) Confronting AIDS: public priorities in a global epidemic. Oxford University Press, New York, USA.
- UN Women (1995) Fourth World Conference on Women Beijing, China - Action for Equality, Development and Peace. UN Women, New York, USA.
- Gill R, Stewart DE (2011) Relevance of gender-sensitive policies and general health indicators to compare the status of South Asian women's health. Womens Health Issues 21: 12-18.
- Duhan R (2014) A study of the status of Indian Women under different Legislations. Innovare journal of Social Science. 2: 2.
- Chacham AS, Maia MB, Greco M, Silva AP, Greco DB (2007) Autonomy and susceptibility to HIV/AIDS among young women living in a slum in Belo Horizonte, Brazil. AIDS Care 19: 12-22.
- United Nations Population Information Network (POPIN) (2016) Guidelines on Women's Empowerment. United Nations Population Information Network (POPIN), UN Population Division, Department of Economic and Social Affairs, UN Population Fund (UNFPA), New York, USA.
- Hackett TM (2011) Domestic Violence against Women: Statistical Analysis of Crimes across India. Journal of Comparative Family Studies 42: 267-288.
- Amin S, Pebley R (1994) Gender Inequality within Households: the Impact of a Women’s Development Programme in 36 Bangladeshi Villages. The Bangladesh Development Studies 22: 121-154.
- UNAIDS (2013) Global Report: UNAIDS report on the global AIDS epidemic. UNAIDS, Geneva, Switzerland.
- Alli F, Maharaj P, Vawda MY (2013) Interpersonal relations between health care workers and young clients: barriers to accessing sexual and reproductive health care. J Community Health 38: 150-155.
- Greig FE, Koopman C (2003) Multilevel analysis of women’s empowerment and HIV prevention: quantitative survey Results from a preliminary study in Botswana. AIDS Behav 7: 195-208.
- Batchelder AW, Gonzalez JS, Palma A, et al. (2015) A Social Ecological Model of Syndemic Risk affecting Women with and At-Risk for HIV in Impoverished Urban Communities. Am J Community Psychol 56: 229-240.
- WHO-HIV Department (2015) Global summary of the HIV/AIDS epidemic 2014. World Health Organization HIV/AIDS Department, Geneva, Switzerland.
- World Economic Forum (2015) Gender Gap Report. World Economic Forum, Geneva, Switzerland.
- Acharya M, Bennett L (1983) Women and the Subsistence Sector: Economic Participation and Household Decision-making in Nepal. World Bank Staff Working Papers 1: 526.
- NIPCCD (2008) A Socio-Cultural Study of Declining Sex Ratio in Delhi and Haryana: A Report. NIPCCD, New Delhi, India.
- Ramesh BM, Gaikwad A, Harangule S, Dhamne S (2010) HIV/AIDS Situation and Response in Maharashtra State Report: Epidemiological Appraisal Using Data Triangulation, published by Director, Communications, India Health Action Trust, Bangalore, India.
- Armstrong G, Nuken A, Medhi GK, Mahanta J, Humtsoe C, et al. (2014) Injecting drug use in Manipur and Nagaland, Northeast India: injecting and sexual risk behaviours across age groups. Harm Reduct J 11: 27.
Citation: Singh SK, Sharma B, Vishwakarma D (2016) Inequalities in the Women’s Empowerment and their Vulnerability to HIV in India. J AIDS Clin Res Sex Transm Dis 3: 007.
Copyright: © 2016 Ana CatShri Kant Singh, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.