Knowledge and Perception towards Hiv/Aids, Tuberculosis and Hepatitis among Serving Corps Members in Nnewi North Local Government: A Cross Sectional Survey
*Corresponding Author(s):
Opeyemi Oluwasanmi AdeloyeUniversity Of Medical Science Teaching Hospital, Ondo, Nigeria
Tel:+234-8145049532,
Email:Adeloyeopeyemi123@gmail.com
Abstract
Abstract
The lack of awareness of several health conditions among people of the community has been on the rise. This study however is aimed at the youths of the society specifically corps members as there is dearth in the evidence on the level of awareness and knowledge in our youth particularly corps members.
Methodology: This study is a cross sectional survey among serving corps members within in Nnewi north local government. Information on knowledge and perception on HIV/AIDS, Tuberculosis and Hepatitis was sort through a structure questionnaire. Descriptive analysis was used in analysing the data obtained.
Results: One hundred questionnaire were distributed but 76 questionnaire were with complete information and analysed, representing 76% response rate, comprising 27(35.5%) male and 49(64.5) female, with a M : F ratio of 1:1.8.Fifteen CDS group participated in the survey, out of which Health and Drug free CDS Group had the highest respondent, health 10(13.2%) and Drug free 9(11.8%) respectively. There was no significant difference between gender and each of HIV/AIDS (χ2=3.388a; p-value = 0.184), Tuberculosis (χ2=4.935a; p-value = 0.177) and Hepatitis (χ2=1.503a ; p-value = 0.472)when p is set at 0.05. However, there was significant association between marital status and each of HIV/AIDS, Tuberculosis and Hepatitis.
Conclusion: The general knowledge and awareness about HIV/AIDS and Tuberculosis was moderate but low for Hepatitis among corps members serving in Nnewi north Local government area. From this study, it appears that more female corps member than their male counterparts are more aware about HIV/AIDS, Tuberculosis and Hepatitis.
Keywords
Awareness; Hepatitis; HIV/AIDs; Tuberculosis
INTRODUCTION
HIV
The human immunodeficiency virus (HIV) is a retrovirus that infects cells of the immune system, destroying or impairing their function. As the infection progresses, the immune system becomes weaker, and the person becomes more susceptible to infections. The most advanced stage of HIV infection is acquired immunodeficiency syndrome (AIDS). It can take 10-15 years for an HIV-infected person to develop AIDS; antiretroviral drugs can slow down the process even further.
Mode of transmission
HIV is transmitted through unprotected sexual intercourse (anal or vaginal), transfusion of contaminated blood, sharing of contaminated needles, and between a mother and her infant during pregnancy, childbirth and breastfeeding.
Research
HIV/AIDS research includes all medical research that attempts to prevent, treat, or cure HIV/AIDS, as well as fundamental research about the nature of HIV as an infectious agent and AIDS as the disease caused by HIV.
Currently, no cure for HIV/AIDS exists. The most universally recommended method for the prevention of HIV/AIDS is to avoid blood-to-blood contact between people and to practice safe sex. The most recommended method for treating HIV is to receive attention from a doctor in charge of coordinating the patient's management of HIV/AIDS [1].
Many governments and research institutions participate in HIV/AIDS research. This research includes behavioral health interventions, such as research into sex education, and drug development, such as research into microbicides for sexually transmitted diseases, HIV vaccines, and antiretroviral drugs. Other medical research areas include the topics of pre-exposure prophylaxis, post-exposure prophylaxis, and circumcision and HIV.
Symptoms of HIV
AIDS symptoms appear in the most advanced stage of HIV disease. In addition to a badly damaged immune system, a person with AIDS may also have; thrush a thick, whitish coating of the tongue or mouth that is caused by a yeast infection and sometimes accompanied by a sore throat severe or recurring vaginal yeast infections, chronic pelvic inflammatory disease severe and frequent infections, periods of extreme and unexplained tiredness that may be combined with headaches, light headedness, and/or dizziness, quick loss of more than 10 pounds of weight that is not due to increased physical exercise or dieting, bruising more easily than normal, long periods of frequent diarrhea, frequent fevers and/or night sweats, swelling or hardening of glands located in the throat, armpit, or groin, periods of persistent, deep, dry coughing, increasing shortness of breath, the appearance of discolored or purplish growths on the skin or inside the mouth, unexplained bleeding from growths on the skin, from the mouth, nose, anus, or vagina, or from any opening in the body, frequent or unusual skin rashes, severe numbness or pain in the hands or feet, the loss of muscle control and reflex, paralysis, or loss of muscular strength, confusion, personality change, or decreased mental abilities.
Preventions
There are many ways you can protect yourself from HIV. The surest way is to abstain from sexual intercourse and from sharing needles and "works" if you use steroids, hormones, or other drugs. Many people have been infected with HIV by sharing needles. If you are using needles for steroids, hormones, or other drugs, Never share needles, Get into a needle-exchange program. Be sure to disinfect the needles you use, Don't share personal items that may have blood on them. This includes toothbrushes, razors, needles for piercing or tattooing, and blades for cutting or scarring, if you choose to have sex, have safer sex to reduce the risk of exchanging blood, semen, or vaginal fluids with your sex partners [2].
Epidemiology
As of 2012 in Nigeria, the HIV prevalence rate among adults ages 15-49 was 3.1 percent. Nigeria has the second largest number of people living with HIV. An estimated population of 3.4 million people living with HIV out of 166.6 million people was recorded.
Tuberculosis
Tuberculosis (TB) is a potentially serious infectious disease that mainly affects your lungs. The bacteria that cause tuberculosis are spread from one person to another through tiny droplets released into the air via coughs and sneezes.
Once rare in developed countries, tuberculosis infections began increasing in 1985, partly because of the emergence of HIV, the virus that causes AIDS. HIV weakens a person's immune system so it can't fight the TB germs. In the United States, because of stronger control programs, tuberculosis began to decrease again in 1993, but remains a concern [3].
Many strains of tuberculosis resist the drugs most used to treat the disease. People with active tuberculosis must take several types of medications for many months to eradicate the infection and prevent development of antibiotic resistance.
Symptoms
Although your body may harbor the bacteria that cause tuberculosis, your immune system usually can prevent you from becoming sick. For this reason, doctors make a distinction between:
- • Latent TB. In this condition, you have a TB infection, but the bacteria remain in your body in an inactive state and cause no symptoms. Latent TB, also called inactive TB or TB infection, isn't contagious. However, it can turn into active TB, so treatment is important for Athe person with latent TB and to help control the spread of TB in general. An estimated one-third of the world's population has latent TB.
- • Active TB. This condition makes you sick and can spread to others. It can occur in the first few weeks after infection with the TB bacteria, or it might occur years later.
Signs and symptoms of active TB
Cough, Unintentional weight loss, Fatigue, Fever, Night sweats, Chills, Loss of appetite
Causes
Tuberculosis is caused by bacteria that spread from person to person through microscopic droplets released into the air. This can happen when someone with the untreated, active form of tuberculosis coughs, speaks, sneezes, spits, laughs or sings.
Although tuberculosis is contagious, it's not easy to catch. You're much more likely to get tuberculosis from someone you live with or work with than from a stranger. Most people with active TB who've had appropriate drug treatment for at least two weeks are no longer contagious [4].
HIV and TB
Since the 1980s, the number of cases of tuberculosis has increased dramatically because of the spread of HIV, the virus that causes AIDS. Tuberculosis and HIV have a deadly relationship — each drives the progress of the other.
Infection with HIV suppresses the immune system, making it difficult for the body to control TB bacteria. As a result, people with HIV are many times more likely to get TB and to progress from latent to active disease than are people who aren't HIV positive.
Epidemiology
Globally there were an estimated 8.7 million incident cases of TB in 2011. There were an estimated 1.42 million deaths. Of these 990,000 were among HIV negative people and there were a further 430,000 deaths among HIV positive people. The incidence of TB per 100,000 people in Nigeria was 118 as of 2011.
Hepatitis
Simply means inflammation of the liver. Hepatitis can heal on its own with no significant consequence, or it can progress to scarring of the liver. Acute hepatitis lasts under six months, while chronic hepatitis lasts longer.
Most liver damage is caused by 3 hepatitis viruses, called hepatitis A, B and C. However, hepatitis can also be caused by alcohol and some other toxins and infections, as well as from our own autoimmune process (the body attacks itself). About 250 million people globally are thought to be affected by hepatitis C, while 300 million people are thought to be carriers of hepatitis B [5].
Not all forms of hepatitis are infectious. Alcohol, medicines, and chemical may be bad for the liver and cause inflammation. A person may have a genetic problem, a metabolic disorder, or an immune related injury. Obesity can be a cause of liver damage which can lead to inflammation. These are known as non-infectious, because they cannot spread form person-to-person.
Fast facts on hepatitis
Here are some key points about hepatitis. More detail and supporting information is in the main article. There are five main types of hepatitis that are caused by a virus, A, B, C, D, and E - plus types X and G. About 250 million people globally are thought to be affected by hepatitis C, while 300 million people are thought to be carriers of hepatitis B. Hepatitis A is caused by eating infected food or water. Hepatitis B is an STD (sexually transmitted disease). Hepatitis C is usually spread through direct contact with the blood of a person who has the disease. Only a person who is already infected with hepatitis B can become infected with hepatitis D. A person can become infected by drinking water that contains HEV (hepatitis E virus). If a hepatitis cannot be attributed to the viruses of hepatitis A, B, C, D, or E, it is called hepatitis X. Hepatitis G is a type of hepatitis caused by the hepatitis G virus (HGV). Initial symptoms of hepatitis are flu-like and may include diarrhea, fatigue, loss of apetite, mild fever, aching, abdominal pain, vomiting, weight loss. How many types of hepatitis are there? There are five main types of hepatitis that are caused by a virus, A, B, C, D, and E - plus types X and G [6].
Hepatitis A
This is caused by eating infected food or water. The food or water is infected with a virus called HAV (hepatitis A virus). Anal-oral contact during sex can also be a cause. Nearly everyone who develops Hepatitis A makes a full recovery - it does not lead to chronic disease.
Hepatitis B
This is an STD (sexually transmitted disease). It is caused by the virus HBV (hepatitis B virus) and is spread by contact with infected blood, semen, and some other body fluids. You get hepatitis B by: Unprotected sexual intercourse with an infected person (unprotected sex means without using a condom) Using a syringe that was previously used by an infected person (most commonly happens with drug addicts and people who inject steroids). Having your skin perforated with unsterilized needles, as might be the case when getting a tattoo, or being accidentally pricked. People who work in health care risk becoming infected by accident in this way. Sharing personal items, such as a toothbrush or razor, with an infected person. A baby can become infected through his mother's milk if she is infected. Being bitten by someone who is infected. The liver of a person infected with hepatitis B swells. The patient can suffer serious liver damage due to infection, resulting in cancer. For some patients the hepatitis becomes chronic (very long-term or lifelong). Donated blood is always tested for hepatitis B [7].
Hepatitis C
Hepatitis C is usually spread through direct contact with the blood of a person who has the disease. It is caused by the virus HCV (hepatitis C Virus). The liver can swell and become damaged. In hepatitis C, unlike hepatitis B, liver cancer risk is only increased in people with cirrhosis and only 20% of hep C patients get cirrhosis. Feces is never a route of transmission in hepatitis C. Donated blood is also tested for hepatitis C. Misuse of anesthesia can result in the transmission of hepatitis B and hepatitis C viruses, researchers reported in the journal Gastroenterology. The cause of infection tends to be from anesthesia contamination, and not endoscopy contamination. Experts say that more effort is needed to better educate the health care community about the importance of strict sterile techniques when using any type of anesthesia.
Hepatitis D
Only a person who is already infected with hepatitis B can become infected with hepatitis D. It is caused by the virus HDV (Hepatitis D Virus). Infection is through contact with infected blood, unprotected sex, and perforation of the skin with infected needles. The liver of a person with Hepatitis D swells [8].
Hepatitis E
A person can become infected by drinking water that contains HEV (hepatitis E virus). The liver swells but there is no long-term consequence. Infection is also possible through anal-oral sex.
Hepatitis X
If a hepatitis cannot be attributed to the viruses of hepatitis A, B, C, D, or E, it is called hepatitis X. In other words, hepatitis of an unknown virus.
Hepatitis G
This is a type of hepatitis caused by the hepatitis G virus (HGV). Usually there are no symptoms. When there are symptoms, they are very mild.
Signs and symptoms
Many people with hepatitis experience either mild symptoms or none at all. Remember that an infected person's feces are always infectious to other people. When symptoms appear, they usually do so about 15 to 180 days after the person has become infected.
The acute phase of hepatitis – symptoms
The initial phase of hepatitis is called the acute phase. The symptoms are like a mild flu, and may include: Diarrhea, Fatigue, Loss of appetite, Mild fever, Muscle or joint aches, Nausea, slight abdominal pain, Vomiting, Weight loss. The acute phase is not usually dangerous, unless it develops into the fulminant or rapidly progressing form, which can lead to death. As the patient gets worse, these symptoms may follow: Circulation problems (only toxic/drug-induced hepatitis) Dark urine, Dizziness (only toxic/drug-induced hepatitis) Drowsiness (only toxic/drug-induced hepatitis), Enlarged spleen (only alcoholic hepatitis), Headache (only toxic/drug-induced hepatitis), Hives, Itchy skin, Light colored feces, the feces may contain pus, Yellow skin, whites of eyes, tongue (jaundice). Patient outcomes after the acute phase depend on various factors, especially the type of hepatitis [9].
Treatments for hepatitis
- • Hepatitis
There are five main types of hepatitis that are caused by a virus, A, B, C, D, and E - plus types X and G.
- • Hepatitis A
There is no treatment specifically for hepatitis A. The doctor will advise the patient to abstain from alcohol and drugs during the recovery. The vast majority of patients with hepatitis A will recover spontaneously.
- • Hepatitis B
A patient with hepatitis B needs to rest. He will require a diet that is high in protein and carbohydrate - this is to repair damaged liver cells, as well as to protect the liver. If this is not enough, the doctor may prescribe interferon. Interferon is an antiviral agent.
- • Hepatitis C
A patient with hepatitis C will be prescribed pegylated interferon and ribavirin.
Patients with chronic hepatitis C who are receiving standard HCV treatment may benefit significantly by taking vitamin B12 supplements, researchers reported in the journal Gut. The authors explained that by adding vitamin B12 to standard treatment, the body's ability to fight the virus is greatly improved. According to their study results, patients who are difficult to treat effectively benefit especially well.
Interferon-free therapy for hepatitis C 'cured' 90% of patients, A new study found that an interferon-free combination of drugs was safe, well tolerated and cured over 90% of 380 trial patients with liver cirrhosis in 12 weeks. The research was published in the New England Journal of Medicine in April 2014 [10].
- • Hepatitis D or E
So far, there is no effective treatment for either hepatitis D or E.
- • Non-viral hepatitis
If the patient has non-viral hepatitis, the doctor needs to remove the harmful substance. It will be flushed out of the stomach by hyperventilation or induced vomiting. Patients with drug-induced hepatitis may be prescribed corticosteroids [11].
How to prevent hepatitis A
- • Wash your hands with soap after going to the toilet
- • Only consume food that has just been cooked
- • Only drink commercially bottled water, or boiled water if you're unsure of local sanitation
- • Only eat fruits that you can peel if you are somewhere where sanitation is unreliable
- • Only eat raw vegetables if you are sure they have been cleaned/disinfected thoroughly
- • Get a vaccine for hepatitis A if you travel to places where hepatitis may be endemic.
How to prevent hepatitis B
- • Tell the partner if you are a carrier or try to find out whether he/she is a carrier
- • Practice safe sex
- • Only use clean syringes that have not been used by anyone else
- • Do not share toothbrushes, razors, or manicure instruments
- • Have a hepatitis B series of shots if you are at risk
- • Only allow well sterilized skin perforating equipment (tattoo, acupuncture, etc.).
How to prevent hepatitis C
- • If you are infected do not let others share your toothbrush, razor, manicure equipment
- • If you are infected cover open wounds
- • Do not share needles, toothbrushes, or manicure equipment
- • If your skin is to be pierced, make sure equipment is well sterilized (tattoo, etc.)
- • Go easy on the alcohol
- • Do not share drug equipment.
How to prevent hepatitis D
- • Use the same guidelines as for hepatitis B. Only a person who is infected with hepatitis B can become infected with hepatitis D.
How to prevent hepatitis E
- • Do the same as you would to protect yourself from hepatitis A infection.
How to prevent alcoholic hepatitis
- • Go easy on the alcohol, or abstain from consuming alcohol.
How to prevent toxic/drug induced hepatitis
- • Make sure you know about the lethal contents of all chemicals
- • Make sure the spray is not pointing at you
- • Make sure you wear protective gear if you have to.
Objectives of the study
The objective of this study is
- • To determine the level of knowledge and perception of corps members on HIV/AIDS, TB and hepatitis.
- • To determine the influence of gender, discipline and marital status on the knowledge and perception of HIV/AIDS, TB and hepatitis.
Motivation of the study
The lack of awareness of several health conditions among people of the community has been on the rise. This study however is aimed at the youths of the society specifically corps members as there is dearth in the evidence on the level of awareness and knowledge in our youth particularly corps members [12].
MATERIALS AND METHODS
Respondents
Respondents that participated in the study were made up of consenting corps members serving in Nnewi north local government.
Inclusion criteria
The respondents were serving corps members and CDS members of Nnewi north local government in Nnewi.
Exclusion criteria
Non-consenting and corps members that were not present were excluded.
Sample size and sampling method
100 respondents were recruited for the study using simple random sampling technique for study in population less than 10,000.
Research Design
This study is a cross sectional survey.
Sites of the study
The respective CDS meeting points of serving corps members within the premises of nnewi north local government.
Instruments
Questionnaires onKnowledge and perception of HIV/AIDS, TB and hepatitis.
Procedure
Approval was sorted and obtained from NYSC office in Nnewi north local government. Upon approval, all the CDS group leaders were briefed about the purpose of the study and their role in the study. Informed consent were obtained from the general CDS members before administering the questionnaire to consenting corps members. Each of the respondents were informed about their rights to withdraw from the study at any point without any consequences. Respondents were assured that the information they provide will be treated with confidentiality and for research purpose only [13].
Data analysis
Descriptive statistics of frequency, percentage, range, mean and standard deviation were used to summarize data. Inferential statistics of chi square test of association was used to determine the influence of demographic parameters on the knowledge and perception of HIV, TB and hepatitis. Data analysis was carried out using SPSS version 16.0 software [14].
Pilot study
A pilot study was conducted among 20 selected corps members to test the validity of the structured questionnaire which was tested valid afterwards.
RESULTS
Distribution of respondent based on demography
One hundred questionnaire were distributed but 76 questionnaire werewith complete information and analysed, representing 76% response rate, comprising 27(35.5%) male and 49(64.5) female, with a M : F ratio of 1:1.8.The majority of respondent were within 23 and 27, 49(64.5%) age group category, 41(53.9%) had science background while 34(44.7%) were Non-Science. 40(52.6%) were married while 36(47.4%) were single. There was no respondent in divorce or widower category respectively [15]. This is shown in (Table 1) below.
|
|
Frequency(N) |
Percentage (%) |
|
|
Gender |
|
||
|
|
Male |
27 |
35.5 |
|
Female |
49 |
64.5 |
|
|
Discipline |
|
|
|
|
|
Science |
41 |
53.9 |
|
Non-Science |
34 |
44.7 |
|
|
ND |
1 |
1.3 |
|
|
Age |
|
||
|
|
18-22 |
4 |
5.3 |
|
23-27 |
49 |
64.5 |
|
|
28-32 |
21 |
27.6 |
|
|
>33 |
1 |
1.3 |
|
|
99 |
1 |
1.3 |
|
|
Marital Status |
|
||
|
|
Married |
40 |
52.6 |
|
Single |
36 |
47.4 |
|
|
Divorce |
0 |
0 |
|
|
Widower |
0 |
0 |
|
Table 1: Shows Demographic distribution of respondent.
Distributon of respondent based on CDS Group
Fifteen CDS group participated in the survey, out of which Health and Drug free CDS Group had the highest respondent, health 10(13.2%) and Drug free 9(11.8%) respectively. Others are Editorial 2(2.6%),Gender 2(2.6%), Cultural 3(3.9%), Educational 3(3.9%) and Service delivery 3(3.9%) CDS groups with the least number of respondent [16].This is shown in (Table 2) below.
|
CDS Group |
Frequency(N) |
Percentage(%) |
|
Agroallied |
5 |
6.6 |
|
Charity |
5 |
6.6 |
|
Culture |
3 |
3.9 |
|
Drugfree |
9 |
11.8 |
|
Editorial |
2 |
2.6 |
|
Education |
3 |
3.9 |
|
EFCC |
6 |
7.6 |
|
Environment |
4 |
5.3 |
|
FRSC |
4 |
5.3 |
|
Gender |
2 |
2.6 |
|
Health |
10 |
13.2 |
|
Legal Aid |
5 |
6.6 |
|
MDGS |
9 |
11.8 |
|
Service delivery |
3 |
3.9 |
|
Sport |
6 |
7.9 |
|
Total |
76 |
100 |
Table 2: Distribution based on CDS group that participated.
Distributon of respondent based on Mean, standard deviation minimum score and maximum score for HIV/AIDS, Tuberculosis and Hepatitis
Table 3 shows the mean overall HIV/AIDS ,Tuberculosis and Hepatitis of respondent. Over 50% of the corps members where moderately knowledgeable about HIV/AIDS and TB with a mean and standard deviation scores of 11.3 and 10.13.40 respectively. However, knowledge about Hepatits was low/poor among corps member with a mean and standard deviation score of 6.76.2. The minimum and maximum score were 2.7 and 17.0, 0.0 and 18.0, 0.0 and 20.0 for HIV/AIDS, Tuberculosis and Hepatitis respectively [17].This is shown in (Table 3) below.
|
|
±Mean (SD) |
Minimum score |
Maximum score |
|
HIV/AIDS |
±11.3 (3.10) |
2.7 |
17 |
|
Tuberculoosis |
±10.1 (3.40) |
0 |
18 |
|
Hepatitis |
±7.7 (6.2) |
0 |
20 |
Table 3: Shows the mean, median, standard deviation, minimum and maximum scores for HIV/AIDS, Tuberculosis and Hepatitis.
Chi square test of association for all respondents between gender and each of HIV/AIDS, Tuberculosis and Hepatitis.
Chi square test of association for all respondent between gender and each of HIV/AIDS, Tuberculosis and Hepatitis. The result shows no significant difference between gender and each of HIV/AIDS(χ2=3.388a; p-value = 0.184), Tuberculosis (χ2=4.935a; p-value = 0.177) and Hepatitis (χ2=1.503a ; p-value = 0.472)when p is set at 0.05 [18]. This is shown in (Table 4) below.
|
|
Low (N) |
Moderate(N) |
High (N) |
χ2 |
P-Value |
|
|
HIV/AIDS |
Male |
6 |
18 |
3 |
3.388 |
0.184 |
|
|
Female |
21 |
25 |
3 |
|
|
|
Tuberculosis |
Male |
5 |
19 |
2 |
4.935 |
0.177 |
|
|
Female |
19 |
28 |
2 |
|
|
|
Hepatitis |
Male |
18 |
3 |
6 |
1.503 |
0.472 |
|
|
Female |
29 |
11 |
9 |
|
|
Table 4: Influence of gender on knowledge and perception HIV/AIDS, tuberculosis and Hepatitis.
Chi-square test of association between Discipline and each of HIV/AIDS, Tuberculosis and Hepatitis
Chi-square test of association between Discipline and each of HIV/AIDS, Tuberculosis and Hepatitis. The result also shows no significant difference between discipline and each of HIV/AIDS(χ2=3.225a; p-value = 0.521), Tuberculosis (χ2=5.855a; p-value = 0.440) and Hepatitis (χ2=11.225a ; p-value = 0.024)when p is set at 0.05. This is shown in (Table 5) below [19].
|
|
Low (N) |
Moderate(N) |
High (N) |
χ2 |
P-Value |
|
|
HIV/AIDS |
Science |
12 |
26 |
3 |
3.225 |
0.521 |
|
|
Non-science |
14 |
17 |
3 |
|
|
|
Tuberculosis |
Science |
10 |
29 |
1 |
5.855 |
0.44 |
|
|
Non-science |
14 |
17 |
0 |
|
|
|
Hepatitis |
Science |
21 |
8 |
14 |
11.225 |
0.024* |
|
|
Non-science |
26 |
6 |
2 |
|
|
Table 5: influence of discipline on knowledge and perception of Tuberculosis.
Chi-square test of association between marital status and each of HIV/AIDS, Tuberculosis and Hepatitis
Chi-square test of association between marital status and each of HIV/AIDS, Tuberculosis and Hepatitis. The result also shows no significant difference between discipline and each of HIV/AIDS (χ2=3.547a; p-value = 0.471), Tuberculosis (χ2=2.943a; p-value = 0.816) and Hepatitis (χ2=0.370a ; p-value = 0.035)when p is set at 0.05 [20] (Table 6).
|
|
Low (N) |
Moderate(N) |
High (N) |
χ2 |
P-Value |
|
|
HIV/AIDS |
Married |
17 |
18 |
3 |
3.547 |
0.471 |
|
|
Single |
9 |
24 |
3 |
|
|
|
Tuberculosis |
Married |
14 |
22 |
0 |
2.943 |
0.816 |
|
|
Single |
10 |
23 |
1 |
|
|
|
Hepatitis |
Married |
18 |
12 |
8 |
0.37 |
0.035* |
|
|
Single |
27 |
7 |
|
|
|
Table 6: Influence of discipline on knowledge and perception of hepatitis.
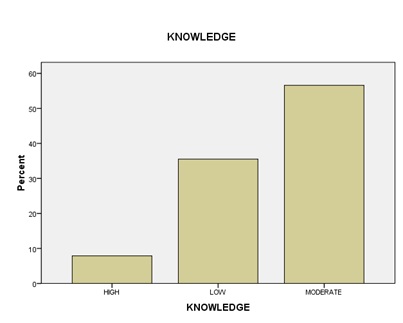 Figure 1: Distribution of corps members based on their knowledge on HIV/AIDS.
Figure 1: Distribution of corps members based on their knowledge on HIV/AIDS.
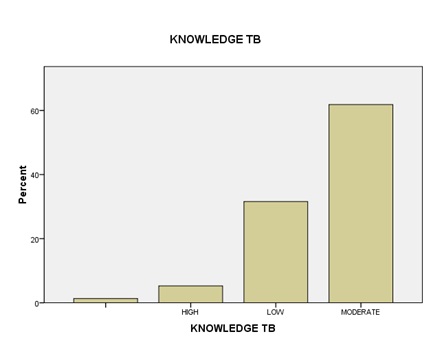 Figure 2: Distribution of corps members based on their knowledge on Tuberculosis.
Figure 2: Distribution of corps members based on their knowledge on Tuberculosis.
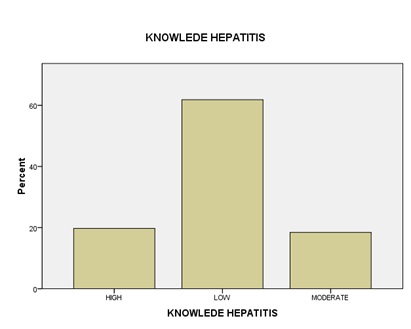 Figure 3: Distribution of corps members based on their knowledge on Hepatitis.
Figure 3: Distribution of corps members based on their knowledge on Hepatitis.
Distribution of corps members based on their perception on HIV/AIDS, Tuberculosis and Hepatitis
(Table 7) shows the distribution of corps members based on their perception on HIV/AIDS, Tuberculosis and Hepatitis. Twelve (15.8%) of respondent thinks “Oral contraceptives can prevent the transmission of HIV”, 14(18.4%) don’t know while 50(65.8%) knew Oral contraceptives can’t prevent the transmission of HIV [21].
|
Characteristic |
Yes(%) |
No(%) |
Don’t Know(%) |
||
|
HIV/AIDS |
Oral contraceptives can prevent the transmission of HIV. |
12(15.8) |
50(65.8) |
14(18.4) |
|
|
Sharing eating utensils with a positive patient can lead to transmission of the disease? |
13(17.1) |
59(77.6) |
4(5.3) |
||
|
Using condom during sex is a reliable protection against HIV/AIDS? |
34(44.7) |
38(50.0) |
4(5.3) |
||
|
I am comfortable being a friend with HIV positive person |
42(55.3) |
21(27.6) |
13(17.1) |
||
|
Tuberculosis |
Is TB contagious |
71(93.4) |
1(1.3) |
4(5.2) |
|
|
If someone has TB will they try to hide it from others? |
18(23.7) |
5(6.6) |
53(69) |
||
|
Do you think it’s shameful to have TB? |
28(36.8) |
30(39.5) |
17(22.3) |
||
|
This is a disease of asocial person? |
25(32.9) |
27(35.5) |
24(31.6) |
||
|
Hepatitis |
Can hepatitis affect any age group? |
38(50.0) |
10(13.2) |
28(36.8) |
|
|
Can hepatitis be transmitted by unsafe sex? |
20(26.3) |
19(25.0) |
37(48.7) |
||
|
Can hepatitis be transmitted through skin? |
9(11.8) |
39(51.3) |
28(36.9) |
||
|
Could you prevent hepatitis transmission? |
41(53.9) |
6(7.90) |
29(38.2) |
||
|
Is vaccination available for hepatitis? |
38(50.0) |
1(1.3) |
37(48.7) |
||
Table 7: Selected Perception of corps member to HIV/AIDS, Tuberculosis and Hepatitis.
CONCLUSION
The general knowledge and awareness about HIV/AIDS and Tuberculosis was moderate but low for Hepatitis among corps members serving in Nnewi north Local government area. From this study, it appears that more female corps member than their male counterparts are more aware about HIV/AIDS, Tuberculosis and Hepatitis. This could be attributed to the fact that more female, than male took part in this study [22].
From this study, discipline was associated with level of knowledge and perception on hepatitis. However, no significant relationship exists between discipline and the knowledge and awareness of HIV/AIDS and Tuberculosis respectively in the studied population. Corps member with science background had better knowledge and perception about Hepatitis but there was no significant difference in their knowledge of HIV/AIDS and Tuberculosis.
Marital status seems to influence awareness level about medical condition among corps members. More married corps members scored higher in the overall knowledge and perception on Hepatitis than single corps members. Married corps member, particularly married female corps member, have cause to visit the clinic either for antenatal, pregnancy screening and they are general believed to be more responsible and such, would be willing to follow their sick relative to the clinic [23].
In conclusion, there is lack/dearth of awareness on hepatitis among corps members. More should be done towards educating corps members on the mode of transmission, pathology, symptoms, vaccination and prevention of these diseases, in particular, hepatitis which is 50 to 100 times more infectious than HIV/AIDS. With this information, great impact will be made towards reducing the scourge associated with the diseases.
RECOMMENDATIONS
From this research, the following are recommended;
- To organise public awareness and enlighten campaign for corps members on HIV/AIDS, tuberculosis and hepatitis. With emphasis on their mode of transmission, pathology, symptoms, vaccination and prevention.
- To conduct free medical test and diagnosis for corps members on these conditions and appropriate medical advice given.
- To organise vaccination programmes on Hepatitis and TB for corps members.
ACKNOWLEDGEMENTS
The health CDS committee acknowledge the NYSC authority, the Nnewi local government zonal inspector and liason inspector for making this study a success. Our esteemed members of the health CDS who gave their support and finally all CDS members that participated in the study.
REFERENCES
- Charles B.U. Uwakwe (2001) Systematized HIV/AIDS education for student nurses at the University of Ibadan, Nigeria: impact on knowledge, attitudes and compliance with universal precautions. JAN 32: 416-424.
- Kumar V, Abbas AK, Fausto N, Mitchell RN (2007) Robbins Basic Pathology (8th ed.). Saunders Elsevier 516-522.
- Konstantinos A (2010) Testing for tuberculosis. Australian Prescriber 33: 12-18.
- World Health Organization (2011) Tuberculosis Fact sheet N°104.
- Warrell, Weatherall DJ, David A (2005) Oxford. Oxford Univ. Press 560.
- Brennan PJ, Nikaido H (1995) The envelope of mycobacteria. Annu Rev Biochem. 64: 29-63.
- Menzies D, Al Jahdali H, Al Otaibi B (2011) Recent developments in treatment of latent tuberculosis infection. Indian J Med Res 133: 257-266.
- Arch G, III Mainous (2010) Management of Antimicrobials in Infectious Diseases: Impact of Antibiotic Resistance. Humana Pr 69.
- Volmink J, Garner P (2007) Directly observed therapy for treating tuberculosis". In Volmink, Jimmy. Cochrane Database Syst Rev.
- Liu Q, Abba K, Alejandria MM, Balanag VM, Berba RP, et al. (2008) Reminder systems and late patient tracers in the diagnosis and management of tuberculosis. Wiley 5: 1206- 1245.
- O'Brien R (1994) Drug-resistant tuberculosis: etiology, management and prevention. Semin Respir Infect 9: 104-12.
- Centers for Disease Control and Prevention (CDC) (2006) Emergence of Mycobacterium tuberculosis with extensive resistance to second-line drugs—worldwide, 2000-2004.
- Maryn McKenna (2012). Totally Resistant TB: Earliest Cases in Italy". Wired.
- Mase S, Chorba T, Lobue P, Castro K (2013) Provisional CDC Guidelines for the Use and Safety Monitoring of Bedaquiline Fumarate (Sirturo) for the Treatment of Multidrug-Resistant Tuberculosis. CDC 62: 1-12.
- World Health Organization (2004) WHO Disease and injury country estimates.
- Lambert M, Hasker E, Deun AV, Roberfroid D, Boelaert M, et al. (2003). Recurrence in tuberculosis: relapse or reinfection?. Lancet Infect Dis 3: 282-287.
- Wang JY, Lee LN, Lai HC, Hsu HL, Liaw YS et al. (2007). "Prediction of the tuberculosis reinfection proportion from the local incidence". J Infect Dis 196: 281-288.
- World Health Organization (2009) The Stop TB Strategy, case reports, treatment outcomes and estimates of TB burden". Global tuberculosis control: epidemiology, strategy, financing. 187-300.
- Centers for Disease Control (2011) Fact Sheets: The Difference Between Latent TB Infection and Active TB Disease.
- Lozano R, Naghavi M, Aggarwal R, Abraham J, Adair T, et al (2012) Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 380 (9859): 2095-2128.
- World Health Organization (2011) Global Tuberculosis Control.
- World Health Organization (2008) Global tuberculosis control.
- FitzGerald JM, Wang L, Elwood RK (2000) Tuberculosis: 13. Control of the disease among aboriginal people in Canada. CMAJ 162: 351-355.
Citation: Adeloye OO (2020) Knowledge and Perception towards Hiv/Aids, Tuberculosis and Hepatitis among Serving Corps Members in Nnewi North Local Government: A Cross Sectional Survey. J AIDS Clin Res Sex Transm Dis 7: 031.
Copyright: © 2020 Opeyemi Oluwasanmi Adeloye, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.