Needle Stick Injuries: ContinuousSurveillance is Essential Task
*Corresponding Author(s):
Avinash KumarConsultant And Head, Department Of Microbiology & Infection Control, The Mission Hospital, Bidhanagar, Durgapur, India
Tel:+ 91-9654876021,
Email:lakchya@gmail.com
Abstract
Needle Stick injuries (NSIs) among Health Care Professionals (HCPs) are one of the significant aspects of any Hospital and it should be monitored continuously and sincerely to prevent blood borne infections. The main objective of this 1 year, annualprospective study is, to be acquainted with the prevalence of NSIs in our tertiary care hospital, so that we can determine risk factors for injury, and do potential interventions for prevention.
Keywords
Blood born viral infections; Health care professionals; Needle sticks injuries;Post exposure prophylaxis
INTRODUCTION
Healthcare Professionals (HCPs)often faces occupational hazard like accidental needle stick injuries (NSIs).The risk of acquiring blood born viral infection like Human Immunodeficiency Virus (HIV), Hepatitis B Virus (HBV) and Hepatitis C Virus (HCV) by NSIs depends on several factors. These factors comprisehollow bore needle, depth of penetration, visible blood on the needle and advanced stage of the disease of the source [1].The important routes in terms of occupational exposure are NSIs (0.3% risk for HIV, 9-30% for HBV and1- 1.8% for HCV)[2].
METHODS
This is an observational prospective annual study done in HCPs of all sections of a Tertiary Care Hospital from May2018 to June 2019.A questionnaire was administered when NSIs were self-reported by HCPs.The questionnaire consists of mode of exposure, depth of injury, immunization status, type of occupation etc.Blood samplesof HCPs exposed by NSIs and of the source, if identified, was collected for baselineHBV, HCV andHIVserum markers. The HCPs who were previously reactive of blood born viral infections were excluded from thisstudy. The exposed HCPs were followed up and repeat testing was done after 3-4 weeks for seroconversion up to 6 months.
RESULTS
The total HCPs reporting NSIs were 25 in which nurses, 09 (36%) Housekeeping, 06 (24%) cleaning staff, 03 (12%), 06 (24%) technicians and 01(4%) Marketing official. Among the staff that had NSIs, 55% had a work experience of less than 1 year. The devices responsible for NSIs were mainly hollow bore needles (56%) (Figure 1).
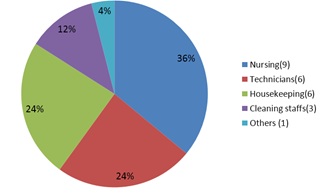 Figure 1: Reported NSIs among HCWs (Total - 25).
Figure 1: Reported NSIs among HCWs (Total - 25).
The patient source was unknown in 06 (24%) of the NSIs.The sex ratio (male/female) was 0.785.The immunization status of victims were 64%(Figure 2).
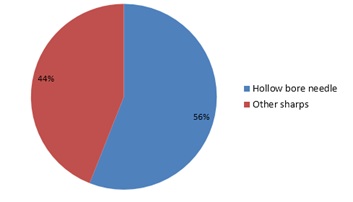 Figure 2: Types of sharps involved.
Figure 2: Types of sharps involved.
Of total source status, 01 was HBs Ag (Hepatitis B surface antigen) and one HCV positive(Figure 3).
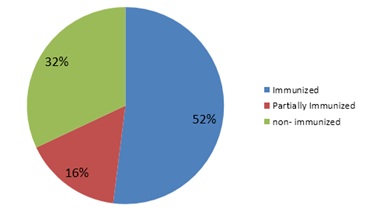 Figure 3: Immunization status of the victim.
Figure 3: Immunization status of the victim.
Recapping of needles caused 25 (8.5%) and other improper disposal of the sharps resulted in 55 (18.6%) of the NSIs(Figure 4).
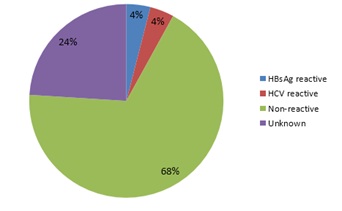 Figure 4: Source of NSIs.
Figure 4: Source of NSIs.
Post-exposure prophylaxis for HCWs who reported injuries was provided immediately. Subsequent 6-month follow-up for human immunodeficiency virus showed zero seroconversion(Figure 5).
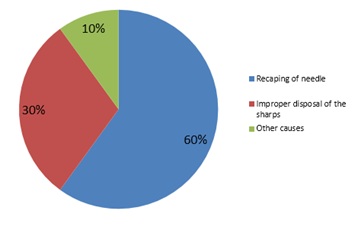 Figure 5: Causes of NSI.
Figure 5: Causes of NSI.
DISCUSSION
As the result itself says, that the NSIs occurred in less experienced, young HCPs, more emphasis should be given for frequent training, education and other precautionary measures.The decision to provide Post exposure prophylaxis (PEP) in our hospital is based on the clinical consideration of risk only. The provision of information regarding PEP was given fullconfidentiality including information about HIV testing, PEP provision and the reasons for seeking PEP. In our study, the practice of recapping needles was found to be most important factor for the cause of NSIsfollowed by others like handling and passing needles or sharps after use, failing to dispose of used needles properly in puncture-resistant sharps containers and poor healthcare waste management practices. In other studies like Ghauri et al. observed 46%, and Alshihry observed 21% cases of NSIs while discarding the needles in comparison to (n = 7; 14%).
In order to reduce NSIs, we are educating and training our HCPs to follow strict compliance to universal work precautions like avoiding injections when safe and effective alternatives are available, avoid recapping needles,plan for safe handling and disposal of needles after use, promptly dispose of used needles in appropriate sharps disposal containers, report all NSIs promptly to ensure that they receive appropriate follow-up care. They participate in training related to infection prevention.The Recording and monitor NSIs with an injury register in each location of healthcare setting is compulsory.All categories of HCPs within the hospital should be trained on how to protectthemselves against HIV and other pathogens transmitted by blood or body fluids. This informationmust be reinforced on a regular basis. All the HCPs must take an individual and collectiveresponsibility in this regard. We conduct hospital infection control meeting quarterly for regular training and monitoring hospital infection control including universal precaution and post-exposure prophylaxis implementation and quality control.
All HCPs must be routinely vaccinated againstthe hepatitis B virus. The vaccination for hepatitis B consists of 3 doses: baseline, 1 month, and6 months. Most of the recipients (99%) seroconvert after completing the full course. There is novaccine or prophylaxis against hepatitis C.The first dose of PEP must be administered ideally within 2 hours (but certainly within the first 72 hours) of exposure and the risk evaluated as soon as possible[3].
CONCLUSION
To conclude, all hospital personnel must have proper awareness regarding risks of NSIs, etiquette for incident reporting, continuous education, safe and sound instrument handling, needle disposal mechanisms, and active participation in ongoing staff training to decrease and prevent occupational hazard [4].
REFERENCES
- Geneva: World Health Organization (2015) Guideline on the use of safety-engineered syringes for intramuscular, intradermal and subcutaneous injections in health-care settings.
- Muralidhar S, Singh PK, Jain RK, Malhotra M, Bala M (2010) Needle stick injuries among health care workers in a tertiary care hospital of India. Indian J Med Res 131:405-410.
- Bidira K, Woldie M, Nemera G (2014) Prevalence and predictors of needle stick injury among nurses in public hospitals of Jimma Zone, South West Ethiopia. Int J Nurs Midwifery 6: 90-96.
- Batra P, MathurP, Bhoi S, Thanbuana BT, Nair S,et al.(2016) Human immunodeficiency virus, hepatitis B virus and hepatitis C virus seroprevalence in critically ill emergency department patients at a Trauma Care Centre, India. Indian J Med Microbiol34: 183-185.
Citation: Kumar A, Das P, Nair VV, Raj RT, Johns V, et al. (2019) Needle Stick Injuries: Continuous Surveillance is Essential Task. J Virol Antiviral 2: 005.
Copyright: © 2019 Avinash Kumar, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.