Review of Properties, Uses and Limitation of TransPalatal Arch (TPA) in Orthodontic Treatment
*Corresponding Author(s):
Doreen MassamuDepartment Of Orthodontics, Lugalo Military Hospital, Dar Es Salaam, Tanzania
Tel:+255759906642,
Email:doreen.johngamaliel256@gmail.com
Abstract
The advancement of technology has brought some successful and progressive innovative methodologies in treating orthodontic conditions such as unilateral cross-bite, protrusive malocclusion, molar derotation, dental asymmetry and premature loss of primary molar teeth. The Trans-Palatal Arch (TPA) is such innovative orthodontic treatment methodologies which have shown impressive treatment results. It comprises of stainless-steel bands around the posterior molar teeth and a looped wire that crosses the mouth palate without touching it. This review covers properties, uses and limitation of TPA in treating orthodontic conditions. Regardless of some limitations in the clinical use of TPA yet it is widely recommended for its various functions as advantages outweigh its limitations.
Keywords
First Molars; Maxilla; Orthodontic; Trans-Palatal Arch
Introduction
Historically in view of correction of different orthodontic conditions, various methods have been applied with progressing successes while others failed to correct the problems. [1] Advancement in technology has brought some innovative methodologies which have been applied and shown impressive improvement in treating some orthodontic conditions like unilateral cross-bite, protrusive malocclusion, molar derotation, dental asymmetry and premature loss of primary molar teeth. The maxillary lingual arch with adjustment loops has been described for use in the upper jaw but are neither common nor familiar to many clinicians and contraindicated only in patients whose bite depth causes the lower incisors to contact the arch wire on the lingual side of the maxillary incisors. [1] A modified maxillary lingual arch described by Nance in 1947 does not contact the anterior teeth, but rather approximates the anterior palate. Nance appliances provide resistance to anterior movement of the posterior teeth and maintain the space effectively. It may cause accumulation of bacteria and food debris often result in palatal and soft tissue inflammation and pain. Poor oral hygiene or distortion of the appliance can lead to palatal tissues hypertrophy and hence soft tissue embedment of the acrylic portion. [1,2] However, the Transpalatal Arch (TPA) a thin wire that goes across the roof of the mouth from right upper first molar to left upper first molar, soldered to molar bands, and runs across the palatal vault, avoid contact with the soft tissue. It follows the vault of the palate, is comfortable, does not interfere with normal speech and avoids palatal soft tissue irritation and inflammation [1,3].
Fashioned to cross the roof of the mouth, TPA has been used in maintaining of arch widths, derotate unilaterally or bilaterally rotated molars, control upper molar eruption, correct unilateral crossbites for maxillary expansion and buccal root torque of upper molars, reinforce anchorage and prevent mesial movement of the upper first permanent molars during treatment and correct mesiodistal asymmetry [2-4] Figure 1 below.
 Figure 1: Transpalatal arch
Figure 1: Transpalatal arch
Due to its closeness to the roof of the mouth, extra care is needed in cleaning around this appliance, by use of floss and the toothbrush, removing food particles and plaque from around this appliance and avoidance of sticky foods can be very beneficial in keeping this appliance in its rightful place [4]. Together with its functions there are some limitations in its uses including anchorage loss, tipping, vertical dimension control, pain, and poor adjustability [5-14]. Therefore, the aim of this review is to discuss properties, different uses and limitations of TPA in orthodontics.
TPA Properties
- TPA Wire Properties
On testing Sagittal and vertical load-deflection and permanent deformation of transpalatal arches connected with palatal implants, Adriano et al., [15] used Stainless steel wires of 6 dimensions: 0.8×0.8, 0.9, 1, 1.1, 1.2, and 1.2×1.2 mm. Absolute orthodontic anchorage without deformation of TPAs was not observed with the wire dimensions tested. To prevent loss of anchorage, wires thicker than 1.2×1.2mm or cast anchorage elements must be considered for clinical practice. However, larger cross sections might cause more patient discomfort, and laboratory procedures increase costs. [15] Forming a passive TPA can be made from stainless steel round wire and should cause no forces, couples or tooth movement once inserted. Widening or narrowing the palatal arch, TPA can be modified to produce a new deactivated shape which can produce a tooth movement once the wire is placed in the attachments by generating force to expand or constrict the intermolar width. The shape produced when the wire is fully engaged in the attachments is the activated shape. Ideally, the activated shape and the passive shape should be identical, so that comfort and soft-tissue contouring are optimal. Adjusting the palatal loop helps to keep the TPA appropriate distance from the palate. TPA can also generate couples through activation of various vbends [16].
- Moment-to-Force Ratio
Balidini and Luder [17] concluded that, moment-to-force ratio increase with increasing arch height and moment-to-force ratio rose with increasing torque. This indicates that when low palatal bars are used, the application of buccal root torque of clinically relevant amounts leads to an initial buccal crown tipping, whereas the same amounts of torque, when applied by means of high arches, bring about an initial buccal root tipping. Therefore, can be concluded that, use of different types of transpalatal arches with different load-deflection rates renders it difficult to get accustomed to the number of compensatory bends necessary for the desired tooth movement and should thus be avoided. Therefore, if heavy arches with a cross section of 0.9 mm and more are used, the buccal root torque bends should not exceed 10 to avoid unnecessary high force delivery.
Functions Of TPA
- Unilateral Cross-bite Correction
The treatment of a unilateral dental crossbite can be performed with a lingual arch in the mandible and TPA in the maxilla. In the case of lingually tipped upper molar, a rigid arch wire is tied to all teeth except the molar in crossbite. Buccal root torque is placed in the TPA on the side that is not in crossbite. When the TPA is inserted into the bracket, the horizontal part of the TPA will be occlusal to the bracket on the crossbite side. In addition, expansion activation should be built in the transpalatal arch. When this TPA is engaged, the force system created causes the desired buccal tipping of the molar in crossbite [18]. Bengt et al., [19] reported a clinical investigation of the correction of the unilateral first molar cross bite with TPA evaluated in 35 children. The outcome of the force system when the TPA was activated for expansion and root torque effectively corrected the crossbite.
- Vertical Molar/Height Control
Transpalatal arch has been found to interfere with the normal vertical descent of the upper molars and therefore retards maxillary vertical alveolar development especially when it is placed low due to the tongue pressure. [20] However, maximum pressure is obtained when the loop of the TPA about 6mm from palate is placed at the middle of the palatal mucous membrane between the right and left second molars. [18] Mark et al., [21] corrected a bimaxillary protrusive malocclusion, complicated by a vertical growth pattern and high mandibular plane angle, with teeth extraction and transpalatal arch to maintain vertical height.
The results were good as the open bite did not express itself, partly due to the use of a transpalatal bar, and occipital headgear and the large amount of ramal growth achieved.
Additionally, Marc et al., [22] performed a retrospective study to examine the skeletal and dental effects of a modified transpalatal bar, dubbed the Vertical Holding Appliance (VHA), used to control the vertical dimension of high-angle patients. Two cephalometrically similar groups of high-angle patients were compared to determine advantages from using the VHA. Lower anterior face height increased more in group II than in group I. The percentage of lower anterior face height to total anterior face height decreased in group I, whereas it increased in group II. The difference between the two groups was determined to be significant. Eruption of the maxillary first molar within group I was less than in group II. Also, Joseph et al., [23] reported the treatment of maxillary skeletal retrusion and severe arch length discrepancy of a 10-year-old boy, of which Edgewise Hawle retainer was placed along with fixed TPA placed on the terminal second molars to prevent further eruption of these teeth until the lower third molars erupted into the occlusion.
- Anchorage
As most of published studies on the use of TPA are case reports, [24-30] in this particular aspect of anchorage, transpalatal arch together with other appliances such as implants, onplants and high pull face bow provided maximum anchorage for maximum retraction of the anterior teeth with successful results in cases with class1 malocclusion, steep mandibular angle, bimaxillary protrusion and a congenitally missing lower left premolar and in class II dental malocclusion of severe overjet, proclination of the maxillary anterior teeth, with minimal crowding. On the other hand, in the management of impacted canine with cantilever, first maxillary molar derotation, maxillary molar intrusion with screws in class II deep overbite and crowding, TPA was used to enhance anchorage with good results. Finally, a study done by Renato et al., [31], to evaluate the distal tipping of partially retracted canines and the mesial movement of the molars with the T-loop, used Passive TPAs and lingual arches of 0.9 mm stainless steel wires to consolidate the left and right segments revealed that the reciprocal moments do not occur in the posterior segment because the force is bilateral, and the moments are canceled since the TPA connects the right and left posterior segments therefore, transforming the several posterior teeth into a large multirooted tooth with 1 Center of Resistance. Small changes in the buccolingual inclinations of the canines can occur because the intrusive force is applied buccally to the Center of Resistance.
- Teeth Derotation/Rotation
It has been shown that mesiopalatally rotated first molars in class1 patient with bimaxillary crowding and in class II malocclusion can be derotated with a transpalatal arch when accompanied by distal force equivalent at the level of maxillary first molar center of resistance and can provide center of rotation approximating lingual attachment. [32-34] This produces an arch gain length of 2.1mm anterior to the molar while simultaneously impinging on maxillary second molar space 1.2mm (per side). However, the derotation is also achieved because of distobuccal rotation and distal tipping of the activated molar of which activated molars moved in a mean distal direction of 1.2mm. However, Edsard et al., [35] stipulated that, rotated molars are frequently seen in the maxillary arch. They further stated that, a mesial-in rotation of one molar can be corrected when a transpalatal arch is used with equal amount of antirotation activations, while at the same time a 0.018x0.025-inch stainless steel wire is tied into all teeth except the rotated molar. Lisa et al., [36] used TPA in rotating and stabilizing maxillary first molars during levelling and alignment and it was removed during canine retraction with minimal loss of posterior teeth anchorage.
And Thomas et al., [37] used TPA to facilitate asymmetric displacement and rotation of upper canines in ankylosed upper left central incisor.
- Maintaining Arch Width
Transpalatal arch has been used to maintain arch width [38-39] after expansion treatment in case with high mandibular plane angle, severe maxillary arch length deficiency, and significant transverse discrepancy. Also, in a patient with unilateral maxillary cross bite, immediately after the removal of rapid palatal expander in a patient with class II division I, anterior openbite and constricted maxilla and in dental and skeletal Class III relationships and maxillary arch-length deficiency. On the other side, Rajendra et al., [40] used TPA to maintain distalized maxillary molar in patients treated by BDA (Biometric Distalize Arch).
- Molar Distalization
Adriano [41] described that, a TPA of Stainless-Steel wire soldered to the palatal implant cap can be used to distalize upper right first molar and correct dental asymmetry. The line of action of the force is through the center of resistance to achieve translation. Ibraham et al., [42] performed a comparison study of 2 distalization systems supported by intraosseous screws, TPA with the intraosseous screw used to distalize maxillary molars with mean distalization of 4.85mm. Also, Seung et al., [43] reported to use TPA with the intraosseous screw to provide anchorage and distalize maxillary arch in bimaxillary protrusive patient. In which maxillary molars were distalized about 5 mm at crown level and 3 mm at apex level. Furthermore, Serhat et al., [44] determined the dentoalveolar and skeletal effects of a TPA in unilateral maxillary first molar distalization, with the treatment group consisted of 15 patients. The maxillary first molars, which were in a dental Class I relationship were the anchorage units, while the molars in Class II relationship (distalized molars) were distalized using a TPA with 150 g of force. The mean unilateral molar distalization was 2.067 mm, with 3.733 distal tipping and 4.800 distopalatinal rotation. The results showed that the TPA was effective in the asymmetric distalization of the maxillary first molars.
- Control Tipping of Posterior Teeth
In correcting occlusal plane canting, openbite and to retract the maxillary dentoalveolar process by using the extraction space of the bilateral maxillary first premolars [10,45-49] a trans palatal arch has been applied to control the transverse tipping, prevent distortion of arch form and buccoversion of posterior teeth that face an intrusion or extrusion force.
- Treatment of Asymmetric Left and/or Right Buccal Occlusion
Often right and left molar relationship is asymmetric. To correct uniarch molar asymmetries a lingual or palatal arch activation is made to deliver a tip forward moment on the Class I side and a tip-back moment on the Class II side. This is a good example where side effects are useful in the correction of the problem [10].
- Arch Expansion
In the correction of class II division 2, Steven [50] inserted a transpalatal appliance into the lingual sheath of maxillary first molars which was activated for mild expansion and rotation with 3.5mm arch width gain. The transpalatal appliance was positioned approximately 2mm off the palate to help maintain the vertical height. Also, Lawrence et al., [51] placed TPA to help widen maxillary arch, in a class II division I malocclusion patient with deep anterior overbite and facial imbalance. Additionally, in Class II division 1 open bite case, David et al., [52] used TPA for molar expansion in which a soldered TPA with expansion was cemented on the first maxillary molars. Similarly, Mikako et al., [53] reported to treat anterior open bite with Skeletal Anchorage System. The upper arch was aligned with progressive expansion by a precision transpalatal arch. The teeth were well aligned and favorable interdigitation was achieved.
- Teeth Intrusion/Extrusion
Transpalatal arch in combination with screws can be used in intrusion of maxillary second molar. In class III pattern, with extruded upper second molar a 2.5mm intrusion of palatal cusps of maxillary second molars with attached hooks to transpalatal arch was achieved [54] Figure 2 below.
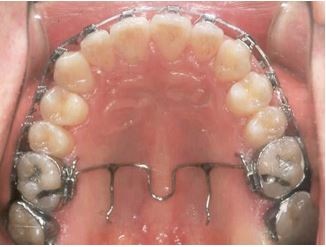 Figure 2: TPA with hooks to intrude second molar
Figure 2: TPA with hooks to intrude second molar
Also, Eve and Winfred [55] stated that, after expansion and retention of maxillary arch with quad-helix in a patient with impacted maxillary canine, a segmental wire attached to TPA was used to further extrude impacted canine which was initially surgically exposed. Additionally, Jae and Tae treated extrusion of the maxillary left first molar because of loss of the mandibular first molar and lingual tilting and rotation of the mandibular second molars by using mini-implants and a TPA with hooks, a 3-mm intrusion was successfully made on the maxillary left first molar [42].
- Space Maintainer
When one or several primary molars are lost, an appliance may be needed to prevent disturbances in the developing dentition. Therefore, the appliance is designed to maintain the relationship among the remaining teeth and guide the eruption of permanent teeth [56].
Limitations of Using TPA
- Anchorage Loss
A study done to evaluate and compare orthodontic anchorage capacity of 4 anchorage systems during aligning and space closure after maxillary premolar extractions showed that, the maxillary molars were stable during the aligning in the Onplant, Orthosystem implant and headgear groups, but the transpalatal bar group had anchorage loss. During the space-closure phase, the molars were still stable in the Onplant and Orthosystem groups, whereas the headgear and transpalatal bar groups had anchorage loss (means, 1.6 and 1.0 mm) respectively [5].
Michael et al., [25] compared the use of onplant supported TPA and without in dogs and monkey to provide anchorage, and results revealed that, TPA without on-plant support had greater loss of anchorage than supported one, with anchorage loss of 1.2mm in anchored molars and 4.1mm in nonanchored molars.
Nevertheless, another study was done in which the finite element method was used to simulate the movement of anchor teeth subjected to mesial forces with and without a TPA. The tipping angles of anchor teeth with and without the TPA were almost the same 28o and 31o respectively. This conclude that, the TPA had no effect on the initial movement. And in the orthodontic movement, the TPA had almost no effect, preserving anchorage for mesial movement as there was 5mm molar mesial movement. [6,7] TPA supported implant used for enhancing anchorage in patients treated with extraction of the maxillary first premolars, anchorage loss of 0.7 mm to 1.1 mm was obtained. [8,27] And Tian et al., [9] performed a study which included growing subjects who required maximum anchorage, headgear and TPA were used and there was average Anchorage loss of 4.3±2.1mm.
- Tipping/Protrusion
In the use of Hilgers pendulum and implant supported TPA to distalize maxillary molars it was found that, Anchorage loss was significant in the pendulum group because of the acrylic button inpalatal depth which is insufficient to resist the reciprocal mesial force of the appliance. Therefore, anchorage loss was seen, especially with the proclination of the maxillary teeth; however, anchorage was not lost in the implant group. The amount of distal tipping of the maxillary first molars was significant in the implant group.8 However, in implant supported TPA used to distalize maxillary molars showed that maxillary molars were rotated distopalatally to a moderate degree, Mild protrusion of the maxillary central incisors was also recorded [10].
- Vertical Dimension Control
John [11] conducted a retrospective cephalometric study of patients with and without transpalatal arches to measure upper molar eruption and its clinical significance to vertical control. The results showed that no statistical difference between control and test group. Gerhard and Frank [12] reported on TPA used in the intrusion of upper left second molar with the anchorage on the first molar. Stating that as a reaction to the intrusive force acting on the second molar, an extrusive force will be exerted on the first molar.
Bucocclusal forces normally are sufficient to prevent first molar extrusion. If antagonist is missing buccal root torque to the TPA at the anchorage tooth is added.
- Pain/Discomfort
Discomfort and pain can be experienced during TPA wear and debonding. This Pain can be relieved by giving analgesics 1hour before treatment [13].
- Poor Adjustability
Modified-TPA shows poor adjustability according to its architecture [14].
Conclusion
Based on the current review, Trans-Palatal Arch is effectively applicable in establishment and maintaining of arch widths, derotate unilaterally or bilaterally rotated molars, control upper molar eruption, correct unilateral crossbites for maxillary expansion and buccal root torque of upper molars, reinforce anchorage and prevent mesial movement of the upper first permanent molars during treatment and correct mesiodistal asymmetry. Implant supported TPA showed to have greater potential to control anchorage than conventional ones. Also, there are some limitations in its uses including, anchorage loss, tipping, protrusion, vertical dimension control, pain, discomfort, and poor adjustability.
Recommendations
Due to the limited information about TPA use in the literature, further studies on the use and limitations of TPA are recommended.
Regardless of some limitations in the clinical use of TPA yet it is widely recommended for its various functions as advantages surpass most of the limitations.
References
- Kupietzky A, Tal E (2007) The Transpalatal Arch: An Alternative to the Nance Appliance for Space Maintenance. Pediatr Dent 29: 235-238.
- Zablocki HL, McNamara JAJr, Franchi L, Baccetti T (2008) Effect of the transpalatal arch during extraction treatment. Am J Orthod Dentofacial Orthop 133: 852-860.
- Stivaros N, Lowe C, Dandy N, Doherty B, Mandall NA (2009) A randomized clinical trial to compare the Goshgarian and Nance palatal arch. Eur J Orthod 32: 171-176.
- Jones LA (2005) Producing smiles Orthodontics PC. USA.
- Feldmanna I, Bondemark L (2008) Anchorage capacity of Osseo integrated and conventional anchorage systems: A randomized controlled trial. Am J Orthod Dentofacial Orthop 133: 19-28.
- Kojima Y, Fukui H (2008) Effects of transpalatal arch on molar movement produced by mesial force: A finite element simulation. Am J Orthod Dentofacial Orthop 134: 1-7.
- Chen F, Terada K, Hanada K, Saito I (2006) Anchorage effect of palatal implants under various forces: A finite element study. Orthodontic Waves 65: 1-8.
- Cousley R (2005) Critical aspects in the use of orthodontic palatal implants. Am J Orthod Dentofacial Orthop 127: 723-729.
- Xu TM, Zhang X, Oh HS, Boyd RL, Korn EL, et al. (2010) Randomized clinical trial comparing control of maxillary anchorage with 2 retraction techniques. Am J Orthod Dentofacial Orthop 138: 1-9.
- Melsen B, Verna C (2005) Miniscrew Implants: The Aarhus Anchorage System. Semin Orthod 11: 24-31.
- Wise JB, Magness WB, Powers JM (1994) Maxillary molar vertical control with the use of transpalatal arches. Am J Orthod Dentofacial Orthop 106: 403-408.
- Kucher G, Welland FJ (1996) Goal-oriented positioning of upper second molars using the palatal intrusion technique. Am J Orthod Dentofacial Orthop 110: 466-468.
- Polat Ö (2007) Pain and Discomfort After Orthodontic Appointments. Semin Orthod 13: 292-300.
- Fujisawa M, Komori A (2010) A modified transpalatal arch with customized bonding base. Orthod Waves 70: 39-42.
- Crismani AG, Celar AG, Burstone CJ, Bernhart TG, Bantleon HP, et al. (2007) Sagittal and vertical load-deflection and permanent deformation of transpalatal arches connected with palata limplants: An in-vitro study. Am J Orthod Dentofacial Orthop 131: 742-752.
- Rebellato J (1995) Two-Couple Orthodontic Appliance System: Transpalatal Arches. Seminars in Orthodontics 1: 44-54.
- Balidini G, Luder HU (1982) Influence of arch, shape on the transverse effects of transpalatal arches of the Goshgarian type during application of buccal root torque. Am J Orrhod 81: 202-208.
- Chiba Y, Motoyoshi M, Namura S (2003) Tongue pressure on loop of transpalatal arch during deglutition. Am J OrthodDentofacialOrthop 123: 29-34.
- Ingervall B, Gollner P, Frohlich K (1995) A clinical investigation of the correction of the unilateral first molar crossbite with the transpalatal arch. Am J Orthod Dentofac Orthop 107: 418-425.
- Kusnoto B, Schneider BJ (2000) Control of the Vertical Dimension. Semin Orthod 6: 33-42.
- Griffies JM, Meyers CE (2000) Treatment of a Class I bimaxillary protrusive malocclusion with a high mandibular plane angle: An American Board of Orthodontics case report. Am J Orthod Dentofacial Orthop 117: 60-67.
- DeBerardinis M, Stretesky T, Sinha P, Nanda RS (2000) Evaluation of the vertical holding appliance in treatment of high-angle patients. Am J Orthod Dentofacial Orthop 117: 700-705.
- Catania JA, Cohen BD, Deeney MR (1990) The use of labial root torque and the tie-forward technique in the treatment of maxillary skeletal retrusion and severe arch length discrepancy. Am J Orthod Dentofacial Orthop 98: 12-18.
- Asscherickx K, Vannet BV, Bottenberg P, Wehrbein H, Sabzevare MM (2010) Clinical observations and success rates of palatal implants. Am J Orthod Dentofacial Orthop 137: 114-122.
- Block MS, Hoffman DR (1995) A new device for absolute anchorage for orthodontics. Am J Orthod Dentofacial Orthop 107: 251-258.
- Liu SY, Herschleb CW (1981) Controlled movement of maxillary incisors in the Begg technique. Am J Orthod 80: 300-315.
- Wehrbein H, Feifel H, Diedrich P (1999) Palatal implant anchorage reinforcement of posterior teeth. Am J Orthod Dentofacial Orthop 116: 678-686.
- Takigawa Y, Sanma Y, Uematsu S, Takada K (2009) The outcome of a two-phase treatment in a patient with Angle Class II, Division 1 malocclusion and an excessive overjet. Orthodontic Waves 68: 88-94.
- Angelle PL (1990) An American Board of Orthodontics case report. Am J Orthod Dentofacial Orthop 98: 285-291.
- GandiniJr LG, Gandini M REAS, Amaral RMDP (2010) Continuous torque system with control of the reaction unit. Am J Orthod Dentofacial Orthop 137: 393-395.
- Martins RP, Buschang PH, GandiniJr LG (2009) Group A T-loop for differential moment mechanics: An implant study. Am J Orthod Dentofacial Orthop 135: 182-189.
- Braun S, kusnoto B, Evans CA (1997) The effect of maxillary first molar derotation on arch length. Am J Orthod Dentofacial Orthop 112: 538-544.
- Haas SE, Cisneros GJ (2000) The Goshgarian Transpalatal Bar. A Clinical and an Experimental Investigation. Semin Orthod 6: 98-105.
- Zachrisson BU, Minster L, Øgaard B, Birkhedd D (2011) Dental health assessed after interproximal enamel reduction: Caries risk in posterior teeth. Am J Orthod Dentofacial Orthop 139: 90-98.
- Steenbergen EV, Nanda R (1995) Biomechanics of orthodontic correction of dental asymmetries. Am J Orthod Dentofacial Orthop 107: 618-624.
- Rajcich MLM, Sadowsky C (1997) Efficacy of Intra arch mechanics using differential moments for achieving anchorage control in extraction cases. Am J Orthod Dentofacial Orthop 112: 441-448.
- Kofod T, Würtz V, Melsen B (2005) Treatment of an ankylosed central incisor by single tooth dento-osseous osteotomy and a simple distraction device. Am J Orthod Dentofacial Orthop 127: 72-80.
- Cureton SL (1998) A significant transverse discrepancy: A case with a high mandibular plane angle, a severe maxillary arch length deficiency, and significant transverse discrepancy. Am J Orthod Dentofacial Orthop 114: 307-310.
- English JD, Olfert KDG (2005) Masticatory Muscle Exercise as an Adjunctive Treatment for Open Bite Malocclusions. Semin Orthod 11: 164-169.
- Rana R, Becher MK (2000) Class II Correction Using the Bimetric Distalizing Arch. Semin Orthod 6: 106-118.
- Crismani AG, Bernhart T, Bantleon HP, Cope JB (2005) Palatal Implants: The Straumann Orthosystem. Semin Orthod 11: 16-23.
- Hyun JM, Kimb TW (2010) Correction of a mutilated dentition with mini-implants as anchorage. Am J Orthod Dentofacial Orthop 138: 656-665.
- Kyung SH, Lee JY, Shin JW, Hong C, Dietz V, et al. (2009) Distalization of the entire maxillary arch in an adult. Am J Orthod Dentofacial Orthop 135: 123-132.
- Eyboúlu S, Bengü AO, Gurton AU, Akin E (2004) Asymmetric Maxillary First Molar Distalization with the Transpalatal Arch. Turk J Med Sci 34: 59-66.
- Kang YG, Nam JH, Park YG (2010) Use of rhythmic wire system with miniscrews to correct occlusal-plane canting. Am J Orthod Dentofacial Orthop 137: 540-547.
- Hashimoto T, Fukunaga T, Kuroda S, Sakai Y, Yamashiro T, et al. (2009) Mandibular deviation and canted maxillary occlusal plane treated with miniscrews and intraoral vertical ramus osteotomy: Functional and morphologic changes. Am J Orthod Dentofacial Orthop 136: 868-877.
- Park HS, Kwon TG, Kwon OW (2004) Treatment of open bite with microscrew implant anchorage. Am J Orthod Dentofacial Orthop 126: 627-636.
- Lioua EJW, Chang PMH (2010) Apical root resorption in orthodontic patients with en-masse maxillary anterior retraction and intrusion with miniscrews. Am J Orthod Dentofacial Orthop 137: 207-212.
- Lai EHH, Yao CCJ, Chang JZC, Chen I, Chen YJ (2008) Three- dimensional dental model analysis of treatment outcomes for protrusive maxillary dentition: Comparison of headgear, miniscrew, and miniplate skeletal anchorage. Am J Orthod Dentofacial Orthop 134: 636-645.
- Emrich SC (1996) An American Board of Orthodontics case report: An adult nonsurgical patient whose treatment required combined dental disciplines. Am J Orthod Dentofacial Orthop 110: 163-169.
- Spillane LM, McNamaraJr JA (1995) Maxillary Adaptation to Expansion in the Mixed Dentition. Seminars in Orthodontics 1: 176-187.
- Gehring D, Freeseman M, Frazier M, Southward K (1998) Extraction treatment of Class II Division I malocclusion with anterior open bite with headgear and vertical elastics. Am J Orthod Dentofacial Orthop 113: 431-436.
- Umemori M, Sugawara J, Mitani H, Nagasaka H, Kawamura H (1999) Skeletal anchorage system for open-bite correction. Am J Orthod Dentofacial Orthop 115: 166-174.
- Jeon YJ, Kim YH, Son WS, Hans MG (2006) Correction of a canted occlusal plane with miniscrews in a patient with facial asymmetry. Am J Orthod Dentofacial Orthop 130: 244-252.
- Tauschea E, Harzer W (2008) Treatment of a patient with Class II malocclusion, impacted maxillary canine with a dilacerated root, and peg-shaped lateral incisors. Am J Orthod Dentofacial Orthop 133: 762-770.
- Harris T, Crawford PJM (2007) Case report: Teeth and tonsils: The use of culture and sensitivity testing for antibiotic prescribing in dental infection. Br Dent J 202: 463-464.
Citation: Massamu D, Machibya F (2023) Review of Properties, Uses and Limitation of TransPalatal Arch (TPA) in Orthodontic Treatment. J Dent Oral Health Cosmesis 8:024
Copyright: © 2023 Doreen Massamu, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.