Rigid Fixed Functional Appliances – A Review
*Corresponding Author(s):
Vivekanand PanzadeDepartment Of Orthodontics, Yogita Dental College And Hospital, Khed, India
Email:drvivekortho5@gmail.com
Abstract
Mandibular retrognathism is the most prevalent skeletal deformity resulting in a class II skeletal pattern. In such cases skeletal changes like anterior repositioning of the mandible is required for achieving an orthognathic profile. Fixed functional appliances have become the key to use the remainder growth in bringing about the skeletal changes alongside dentoalveolar changes. Thus the knowledge of these appliances would benefit the orthodontist to establish a selection criteria of a specific appliance most suitable for the patient.
Introduction
The number of Class II patients reporting to an Orthodontist’s office for treatment is quite significant. Mandibular retrusion contributes to a majority of these Class II malocclusions. For a post-pubertal patient orthodontic camouflage or surgical options were considered and modulating growth was considered improbable. However, studies on young adults by Pancherz [1] and co-workers have demonstrated the potential of condylar and glenoid fossa remodeling beyond the pubertal growth spurt using the Herbst appliance. Fixed functional appliances or more appropriately termed ‘non-compliant Class II inter-arch correctors’ have gained significant ground.
The main advantages of combining Fixed functional treatment along with fixed appliance therapy is termed as “Telescoping treatment”. This refers to the combination of two treatment modalities to maximize the benefits whilst minimizing their individual drawbacks. To be more specific, the fixed appliance is aimed at targeting the dentition and providing the following dental corrections: a) facilitating mandibular advancement by eliminating dental interferences and b) consolidating the arches in order to minimize the adverse dental side-effects. This is in conjunction with the fixed functional appliance providing the impetus for anterior mandibular repositioning and optimizing growth.
Evolution Of Fixed Functional Appliances
The first fixed functional appliance namely, the Herbst appliance, was very rigid, suffered from breakages and could allow for only limited lateral movements. Operators had difficulties in placing the appliance and patients found it difficult to cope up with. Appliances similar to Herbst have been labeled as rigid fixed functional appliances. As an alternative, the Jasper Jumper [2] was subsequently introduced, which solved the issue of patient comfort but continued to break very often. This was mainly attributed to the curvilinear stresses generated when the spring of the Jasper was flexed intra-orally. Class II correctors belonging to this category have been branded as Flexible fixed functional appliances. The Jasper Jumper also showed more dento-alveolar changes in effecting the Class II correction and was considered a disadvantage in comparison to Herbst, which had demonstrated more orthopedic changes. This led to the evolution of the Hybrid fixed functional appliances or Inter-arch compression springs (Table 1).
- Classification of Fixed Functional Appliances
|
RIGID |
FLEXIBLE |
HYBRID |
Appliances Acting as Substitutes for Elastics |
|
Herbst and variants Goodman’s Modified Herbst Appliance Mandibular Advancement Locking Unit (MALU) Magnetic Telescopic Device Flip-Lock Herbst Appliance Hanks Telescoping Herbst Appliance Ventral Telescope Universal Bite Jumper IST (Intraoral Snoring Therapy) Appliance Acrylic Splint with Hinge System Cantilever Bite Jumper (CBJ) Molar-Moving Bite Jumper (MMBJ) Mandibular Advancing Repositioning Splint (MARS) Mandibular Corrector Appliance (MCA) MPA (I – IV) FOMA II Ritto appliance Biopedic appliance MARA Rick-A-Nator Fixed magnetic appliance Functional mandibular advancer AdvanSync |
Jasper Jumper Adjustable Bite Corrector Churro Jumper Amoric Torsion coils Scandee tubular jumper Bite fixer Klapper SUPERspring II Gentle Jumper Flex developer Ribbon Jumper Forsus Nitinol Flat Spring |
Twin Force Bite Corrector (TFBC) Forsus Fatigue-Resistant Device Sabbagh Universal Spring (SUS) Eureka Spring Powerscope Vibhute Class II corrector |
Calibrated Force Module Alpern Class II Closers Saif Springs Herbst with force module |
Table 1: Classification of Fixed Functional Appliances.
Herbst Appliance: The Herbst appliance (Figure 1) is a fixed appliance which functions like an artificial joint between the maxilla and the mandible. The original design (banded Herbst design) consists of a bilateral telescopic mechanism attached to orthodontic bands on maxillary first permanent molars and on mandibular first premolars, which maintains the mandible in a continuous protruded position [1].
A more recent version of the Herbst appliance was developed by Pancherz, in which the bands are replaced by cast splints (cast splint Herbst design), which fit precisely and cover the teeth in their lateral segments, fabricated from cobalt-chromium alloy and cemented with glass ionomer cement to the teeth. Each of the telescopic mechanisms consists of a tube and a plunger which fit together, two pivots and two locking screws. The pivot for the tube is soldered to the maxillary first molar band and the pivot for the plunger to the mandibular first premolar band. The tubes and plungers are attached to the pivots with the locking screws and can easily rotate around their point of attachment. The bands on which the tube and the plunger are attached should be fabricated from at least 0.15 mm or 0.010′′ thick orthodontic material, which prevents any breakage during treatment with the Herbst appliance and also allows increased extension in the occlusocervical direction to achieve adequate retention of the bands on the teeth [3].
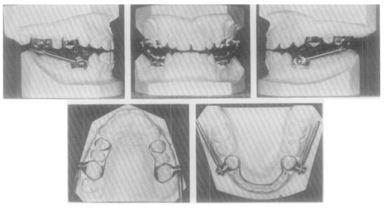 Figure 1: Different views of the Herbst appliance
Figure 1: Different views of the Herbst appliance
- Variants of Herbst Appliance
Acrylic Splint Herbst Appliance: The Acrylic Splint Herbst Appliance (Figure 2) consists of the telescopic mechanism which is attached to acrylic splints cemented or bonded on the maxillary and mandibular dentition. For the attachment of the bite-jumping mechanism, a wire framework is used, over which 2.5–3 mm acrylic is adapted. A transpalatal arch or, more usually, a rapid palatal expansion screw attached to the wire framework connects the left and right parts of the splint together. The acrylic maxillary and mandibular splints can also be removable. The appliance can be worn on a full-time basis and removed only for oral hygiene, or on a part-time basis. Mainly due to the fact that bonding of the acrylic splints increases the risk of decalcification [4].
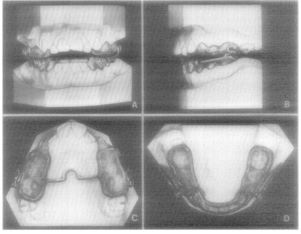 Figure 2: Acrylic Splint Herbst Appliance - A through D, Trimmed Herbst appliance after final polish. In this case the acrylic extends only to the lingual surface of the upper canine, the design used when the maxillary splint is bonded.
Figure 2: Acrylic Splint Herbst Appliance - A through D, Trimmed Herbst appliance after final polish. In this case the acrylic extends only to the lingual surface of the upper canine, the design used when the maxillary splint is bonded.
Goodman’s Modified Herbst Appliance: This appliance (Figure 3) consists of stainless steel crowns placed on the maxillary first permanent molars and, if additional anchorage is required on maxillary first deciduous molars, a transpalatal arch fabricated from 0.045′′ round wire connecting the crowns, bands on the mandibular first molars, frameworks for both mandibular and maxillary arches made of 14-gauge half-round wire, and the Herbst telescopic mechanism. The maxillary pivots are soldered to the most distobuccal points of the crowns, parallel to the distal and the occlusal surfaces, while the mandibular pivots are soldered to the wire framework on a level with the mesial surface of the first deciduous molars. A wax-bite in an edge-to-edge incisal position is taken and the cementation of the appliance follows after a trial procedure [5].
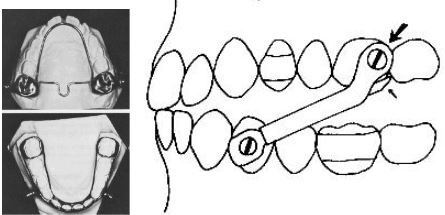 Figure 3: Small arrow shows 45° cut at end of arm extension, mesial to maxillary second molar. Large arrow shows screw where ratcheting may occur if parallelism is not achieved or patient makes repetitive, forceful lateral excursions.
Figure 3: Small arrow shows 45° cut at end of arm extension, mesial to maxillary second molar. Large arrow shows screw where ratcheting may occur if parallelism is not achieved or patient makes repetitive, forceful lateral excursions.
Mandibular Advancement Locking Unit (MALU): The Mandibular Advancement Locking Unit (Figure 4) was introduced by Schiavoni et al and consists of two tubes, two plungers, two upper “Mobee” hinges with ball-pins, and two lower key hinges with brass pins. Bands are placed on the maxillary first molars with 0.051′′ headgear tubes, while a palatal arch can be used in cases of overexpansion. Regarding the mandible, bands are placed on the mandibular first molars, while the anterior teeth are bonded from canine to canine with 0.022′′ brackets, and a 0.021 × 0.025′′ stainless steel archwire with labial root torque in the anterior section is used, bent back at the distal ends. The Mobee hinge is inserted into the hole at end of the MALU tube and secured to the first molar headgear with the ballpin, while the lower key hinge is inserted into the hole at the end of the plunger and locked to the mandibular base arch with the brass pin. The length of the tube–plunger assembly is specified by the amount of mandibular advancement required, and further advancements of 1–5 mm can be performed using spacers [6].
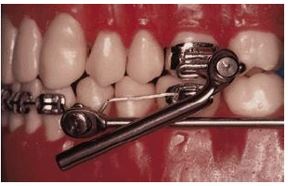 Figure 4: Mandibular Advancement Locking Unit - With upper and lower MALU components in place, length of tube-plunger assembly is adjusted according to desired mandibular protrusion.
Figure 4: Mandibular Advancement Locking Unit - With upper and lower MALU components in place, length of tube-plunger assembly is adjusted according to desired mandibular protrusion.
Magnetic Telescopic Device: According to Ritto, the Magnetic Telescopic Device consists of two tubes and two plungers with a semicircular section and with NdFeB magnets, which are positioned to exert a repelling force, while fitting is achieved using the MALU system. Its main advantages include the linking of a magnetic field on a functional appliance, while its disadvantages involve its thickness, the laboratory work necessary to prepare it, and the covering of the magnets [7].
Flip-Lock Herbst Appliance: The Flip-Lock Herbst Appliance (Figure 5) uses ball-joint connectors instead of screw attachments, and it needs no retaining springs. The ball-joint connectors are attached to stainless steel crowns on maxillary first molars and mandibular first premolars. Further, bands are placed on mandibular first molars and a lingual arch connects them with the crowns on first premolars. The rods have forked ends to be crimped onto the mandibular balls [8].
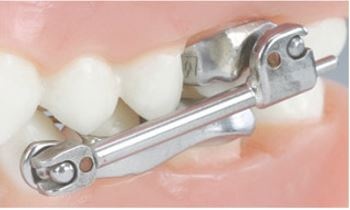 Figure 5: Flip-Lock Herbst Appliance
Figure 5: Flip-Lock Herbst Appliance
Hanks Telescoping Herbst Appliance: It consists of two tubes, a ball and socket joint, and a rod attached to the mandibular premolars or cantilever arms, and functions like a free-sliding radio antenna. The outer tube of the axle captures the middle tube and the middle tube slides inside the outer tube stopped at the mesial end of the outer tube. The rod is captured by the middle tube and slides inside the middle tube until it is stopped at the mesial end of the middle tube (Figure 6). The advantages of the Hanks Telescoping Herbst include one-piece design, which prevents disengagement, reduced ulcerations, greater lateral movements of the mandible because of the ball and socket joints, fewer emergency appointments, patient comfort and user friendly components [9].
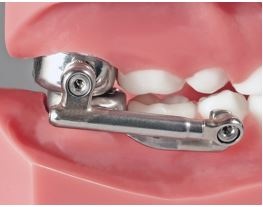 Figure 6: Hanks Telescoping Herbst
Figure 6: Hanks Telescoping Herbst
Ventral Telescope: The Ventral Telescope is first intermaxillary appliance fabricated as a single unit and is fixed via ball attachments. The Ventral Telescope is available in two sizes and is activated by unscrewing the tube, thereby causing approximately 3 mm of activation. Its advantages include elimination of the risk of the appliance disassembling when maximum opening occurs, and easy and simple operation, while its disadvantages include thickness and fractures of the brake which stabilizes the joint [10].
Universal Bite Jumper: The Universal Bite Jumper (Figure 7) was introduced by Calvez and is similar to the Herbst appliance but smaller and more adaptable, while an active coil spring can be added when needed. The jumper is fitted in the mouth and cut to the proper length depending on the amount of mandibular advancement. The activation is achieved by crimping 2–4 mm crimping bushes onto the rods, whereas when coil springs are used, no activation is required [11].
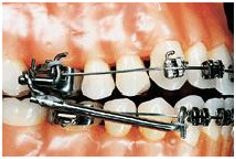 Figure 7: Universal Bite Jumper
Figure 7: Universal Bite Jumper
Open-Bite Intrusion Herbst Appliance: The Open-Bite Intrusion Herbst (Figure 8) for mixed dentition consists of a maxillary and a mandibular part. The maxillary part consists of crowns cemented on the maxillary second deciduous molars and permanent first molars, stops which extend from the deciduous second molars to the deciduous first molars, 0.036′′ stainless steel intrusion wires with helix loops soldered to the deciduous second molars to intrude the maxillary permanent first molars, cantilever extensions with 0.022′′ archwire tubes soldered to the deciduous second molar crowns, and positioning axles distal to the deciduous second molar crowns and just mesial to the permanent first molar crowns. The telescopic axles are initially soldered to the axles to maintain the position of the primary second molars while intruding the permanent first molars, while axles positioned to the first molar crowns are used to connect the Herbst mechanism and maintain the intruded molars during Class II correction [12].

Biopedic Appliance: The Biopedic designed by Collins, was introduced in 1997 and consists of buccal attachments soldered to mandibular and maxillary first molar crowns. The attachments contain a standard edgewise tube and a 0.070′′ molar tube, while large rods pass through the tubes. The maxillary rod, which is inserted from the distal, is fixed by a screw clamp mesial to the maxillary first molar, while the mandibular rod is inserted from the mesial of the molar tube and is fixed at the distal by a similar screw. The rods are connected via a rigid shaft, while two pivots on their ends allow the appliance to be rotated when the patient opens his mouth. The Biopedic appliance is activated by moving the mandibular rod mesially and fixing the screw [17].
Ritto Appliance: The Ritto Appliance (Figure 12) was developed by Ritto and is described as a miniaturized telescopic device with simplified intraoral application and activation. It is a one-piece device with telescopic action, which is fabricated in a single format able to be used bilaterally, attached to upper and lower archwires. A steel ball-pin and a lock-controlled sliding brake are used as fixing components. In addition, two maxillary and two mandibular bands and brackets on the mandibular arch can support the appliance adequately. The appliance is activated by sliding the lock around the lower arch distally and fixing it against the appliance. The activation is performed in two steps, an initial adjustment activation of 2–3 mm and a subsequent activation of 1–2 mm 1 week later, while further activations of 4–5 mm can be performed after 3 weeks [18]. 
Figure 12: Ritto Appliance
Mandibular Anterior Repositioning Appliance (MARA): The MARA is attached to stainless steel crowns or rigid bands on the first molars. In addition to the normal rectangular archwire tube, the upper first molar has a large .062 square tube, into which slides an adjustable .060 square “elbow” that hangs vertically. The lower first molar has the normal rectangular tube as well as an .059 round wire “arm” projecting buccally from the mesial. The upper elbow hits the lower arm and prevents occlusion unless the patient holds the lower jaw forward so that the lower arm is in front of the elbow. In the occluded position, the elbow and arm shield each other and prevent irritation of the cheek. The lower crowns or bands are stabilized by either a lingual arch or lower braces to prevent unwanted mesiolingual rotation of the lower molars resulting from the resting pressure of the elbows (Figure 13). The elbows are advanced periodically by placing shims on them in order to cause more mandibular advancement (the elbows are tied in by ligatures (Figure 8)) [19]. 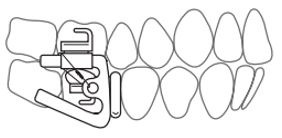
Figure 13: Mandibular Anterior Repositioning
Mandibular Protraction Appliance (MPA): The Mandibular Protraction Appliance was introduced by Coelho Filho for the correction of Class II malocclusion. It has been continuously developed since its initial introduction and four different types have been proposed (Figures 14-16), all by Coelho Filho [20,21]. 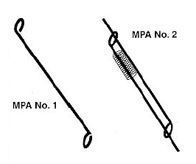
Figure 14: MPA No. 1 & 2
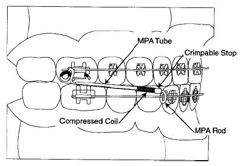 Figure 15: MPA No. 3
Figure 15: MPA No. 3
 Figure 16: MPA No. 4
Figure 16: MPA No. 4
Functional Mandibular Advancer (FMA): The FMA (Figure 17), which was developed by Kinzinger et al., as an alternative to the Herbst appliance for the correction of Class II malocclusions, is a rigid intermaxillary appliance based on the principle of the inclined plane. It is similar to the MARA but with some fundamental differences. It consists of cast splints, crowns or bands on which the main parts of the appliance, the guide pins and inclined planes, are laser welded buccally. The bite-jumping appliance of the FMA is attached at a 60° angle to the horizontal, thus actively guiding the mandible in a forward position while closing, which provides unrestricted mandibular motion and increases patient adaptation. According to Kinzinger et al., the anterior shape of the bite-jumping device and the active components of the abutments were designed to allow mandibular guidance even in partial jaw closure, thus ensuring its effectiveness even in patients with habitual open mouth posture. The appliance is reactivated by adjusting the threaded insert supports over a length of 2 mm, using guide pins of different width or by fitting the sliding surfaces of the inclined planes with spacers of different thicknesses. Therefore, the mandibular advancement can be accomplished following a step by-step procedure which provides better patient adaptation, especially for adult patients [22].
 Figure 17: Functional Mandibular Advancer
Figure 17: Functional Mandibular Advancer
Functional Orthopedic Magnetic Appliance (FOMA) II: Functional Orthopedic Magnetic Appliance II (NeFeBo) has upper and lower attracting magnets. Active appliance, directs its inherent magnetic forces to the jaws, thereby keeping the jaw in an advanced posture. The lower magnetic housing was incorporated into the lower plate on the dental model. Both upper and lower plates were then bonded to the dental arches. The two magnets are fully superimposed with no air gap. Before monthly reactivation, the upper magnet was separated from the upper plate and similarly reattached [23].
Rick-A-Nator Appliance: The Rick-A-Nator (Figure 18) consists of two molar bands on the upper first permanent molars and an anterior acrylic bite plate which is fabricated from self-cure acrylic resin. This anterior bite plane is converted into an anterior repositioning appliance by the addition of acrylic incisal ramp. The acrylic incisal ramp engages the lingual of the anterior teeth and so, the lower teeth bite into a forward bite relationship. The anterior inclined plane guides the mandible forward into a class I relationship as the patient closes. The anterior acrylic is connected to the molar bands by 0.045 stainless steel connector wires. Rests can be added on primary molars or first bicuspids to increase the stability of the appliance [24].
 Figure 18: Rick-A-Nator appliance design
Figure 18: Rick-A-Nator appliance design
AdvanSync: AdvanSync appliance is a recent modification of the Herbst appliance, also known as Molar to Molar appliance. AdvanSync was developed by Terry and Bill Dischinger in 2008 for treating skeletal class II malocclusion. The AdvanSync (Figure 19) is a fixed tooth-born functional appliance consisting of crowns cemented on maxillary and mandibular permanent first molars, a position where orthopedic forces are applied. It shows more headgear effect but less mandibular length enhancement. The telescopic mechanism acts to constantly posture the mandible forward upon closure, with the goal of enhancing mandibular growth. It is designed to allow simultaneous fixed orthodontic appliance treatment. (0.0220 ×0.0280) slot edgewise bracket system is fully bonded with the brackets on the mandibular incisors having a built-in labial root torque [25].
 Figure 19: AdvanSync
Figure 19: AdvanSync
Conclusion
Conventional orthodontic appliances use mechanical force to alter the position of teeth into a more favorable position. However, the scope of these fixed appliances is greatly limited by certain morphological conditions of the orofacial skeleton wherein modifications are required to the sagittal discrepancies. To overcome this limitation, functional appliances came into existence. Non-compliant patients were further effectively managed by fixed functional appliances. According to Pangrazio et al., removable or fixed functional appliances bring about sagittal and vertical skeletal changes in the jaw positions resulting in orthopaedic and orthodontic changes [26]. In contrast to removable appliances, which have an “intermittent” mode of action, the fixed ones work “continuously”. Class II correction with a fixed functional appliance is a combination of skeletal and dentoalveolar changes, by exploiting the remaining growth in the craniofacial structures. Thus fixed functional appliances are a useful addition to the orthodontic armamentarium.
References
- Pancherz H (1979) Treatment of Class II malocclusions by jumping the bite with the Herbst appliance: A cephalometric investigation. Am J Orthod 76: 423-442.
- Jasper JJ (1987) The Jasper Jumper – a fixed functional appliance. Sheybogan: American Orthodontics, USA.
- Pancherz H (1985) The modern Herbst appliance – its biologic effects and clinical use. Am J Orthod 8: 1-20.
- McNamara JA (1988) Fabrication of the acrylic splint Herbst appliance. Am J Orthod Dentofacial Orthop 94: 10-18.
- Goodman P, McKenna P (1985) Modified Herbst appliance for the mixed dentition. J Clin Orthod 19: 811-814.
- Schiavoni R, Bonapace C, Grenga V (1996) Modified edgewise-Herbst appliance. J Clin Orthod 30: 681–687.
- Ritto AK (1997) Tratamento das Classes II divisão 1 com a Biela Magnética. Universidade do Porto. Reitoria.
- Miller RA (1996) The flip-lock Herbst appliance. J Clin Orthod 30: 552-558.
- Hanks SD (2003) Herbst therapy: trying to get out of the 20th century. Good Practice Newsletter of 4: 2–4.
- Ritto AK, Ferreira AP (2000) Fixed functional appliances - a classification. Funct Orthodontic 17: 12-32.
- Calvez X (1998) The universal bite jumper. J Clin Orthod 32: 493-500.
- Dischinger TG (2001) Open-bite intrusion Herbst. AOA Orthodontic Appliances 5: 1-6.
- Faulkner J (1997) An interview with Dr. Joe Mayes on the Cantilever Bite Jumper. Orthodontic CYBER journal.
- Mayes JH (1998) The molar-moving bite jumper (MMBJ). Clinical Impression 7: 16-19.
- Clements RM Jr, Jacobson A (1982) The MARS appliance. Report of a case. Am J Orthod 82: 445-455.
- Jones M (1985) Mandibular corrector. J Clin Orthod 19: 362–368.
- Graber TM, Vanarsdall RL (1994) Orthodontics: Current principles and techniques. Mosby: 965.
- Ritto AK (1999) Fixed functional appliance – trends for the next century. Funct Orthod 16: 22-39.
- Eckhart JE (1998) Introducing the MARA. Clin Impressions 7: 2–27.
- Filho CMC (1997) Clinical applications of the Mandibular Protraction Appliance. J Clin Orthod 31: 92-102.
- Filho CMC (1998) The Mandibular Protraction Appliance No. 3. J Clin Orthod 32: 379-384.
- Kinzinger G, Ostheimer J, Forster F, Kwandt PB, Reul H, et al. (2002) Development of a new fixed functional appliance for treatment of skeletal class II malocclusion first report. J Orofac Orthop 63: 384-399.
- Vardimon AD, Stutzmann JJ, Graber TM, Voss LR, Petrovic AG (1989) Functional orthopedic magnetic appliance (FOMA) II—Modus operandi. Am J Orthod Dentofac Orthop 95: 371-387.
- Papadopoulos MA (2006) Orthodontic Treatmentof the Class II Noncompliant Patient. Mosby: 7-9.
- Dischinger BM (2018) Skeletal class II case presentation: utilization of the Advansync 2 appliance. APOS Trends in Orthodontics 8: 168–174.
- Pangrazio-Kulbersh V, Berger JL, Chermak DS, Kaczynski R, Simon ES, et al. (2003) Treatment effects of the mandibular anterior repositioning appliance on patients with Class II malocclusion. Am J Orthod Dentofacial Orthop 123: 286-295.
Citation: Panzade V, Patil C, kawale P, Sonone T, Joshua B, et al. (2023) Rigid Fixed Functional Appliances – A Review. J Dent Oral Health Cosmesis 8:22
Copyright: © 2023 Vivekanand Panzade, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.