Risky Sexual Behaviors and Associated Factors among Mizan, Bonga and Tepi Preparatory School Students, Southwestern, Ethiopia, 2016: A Cross Sectional Study
*Corresponding Author(s):
Tensay KahsayDepartment Of Nursing, College Of Health Sciences, Mekelle University, Mekelle, Ethiopia
Tel:+251 912937986,
Email:tensay1221@gmail.com
Abstract
Methods: Institution based cross-sectional study was conducted by employing both quantitative and qualitative data collection method from November 1 to December 30, 2016. Systematic random sampling technique was employed for study participant selection. Quantitative data was collected by self-administer questionnaire whereas an in-depth interview was used for qualitative data. Descriptive, logistic regression analysis was performed during data analysis.
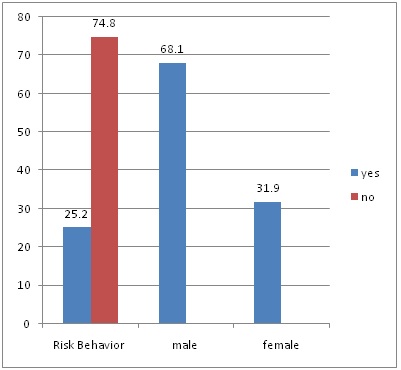
Results: The overall risky sexual behavior was found to be 25.2% (119 out of 473). Living away from their parent, students who did not attend religious programs, alcohol drinkers, pornography watchers and monthly family income less than 900 birr were found to be predictors of risky sexual behavior of the participants.
Conclusion: This study revealed that there is a risky sexual behavior among Mizan, Bonga and Tepi preparatory school students. Therefore responsible bodies should take the initiative to bring about healthy sexual behaviors among school youths.
Keywords
ABBREVIATIONS
AOR: Adjusted Odd Ratio
HIV: Human Immune Deficiency Virus
WHO: World Health Organization
FGD: Focus Group Discussion
STI: Sexually Transmitted Infections
INTRODUCTION
One-fifth of the world's population includes adolescent and young adults, with more than four-fifths in developing countries. During the transition from childhood to adulthood, youth establish patterns of behavior and make lifestyle choices that affect both their current and future health [5]. Today’s adolescent and young adults constitute the largest cohort ever to enter the transition to adulthood. Evidence showed that nearly half of the global populations were less than 25 years old and nearly 90% live in developing countries. In Ethiopia 45% of the population under age 15 and 71% under age of 30 years [6]. Adolescence is characterized by emotional, social and physical transformations that can expose young people to emotional and health vulnerabilities. In this period of development, young people begin to engage in risky behaviors, such as alcohol/drug use and unsafe sex [7].
Adolescence is a critical developmental period when many youth begin to define and clarify their sexual values and start to experiment with sexual behaviors. Most of these youth are students and they are also at a high risk for unsafe sexual behaviors and problems like HIV/AIDS or STI (Sexually Transmitted Infections), unwanted pregnancy, abortion, poor school performance, high school dropout rate, psycho-social problems, conduct disorder, divorce and economic problems [8,9]. Sexual behavior and reproductive health of youth in developing countries have attracted a considerable attention over the last 15 years. But, a large proportion of the population in these countries is affected by HIV/AIDS and reproductive health problems. The sexual behavior of youth is important not only because of the possible reproductive outcomes but also because of the fact that risky sexual behavior is associated with sexually transmitted infections [10,11].
METHOD
Study area
Study design and Sample size determination
Data collection
Specifications of variables
Living out of parents: Living away from parent rented may be due to distance and others.
Predisposing factor: Any condition related to biology, cultural, economic, demographic or personal that can increase the risk of involving in risky sexual behavior.
Risky sexual behavior: Those who have one of the following: having more than one sexual partner, performing sexual intercourse with non-regular partner without condom and having sex with commercial sex worker.
Substance use: Use of at least any one of the following substances: alcohol, khat, cigarette shisha, hashish or drug that are assumed to motivate and increase risk of involving in risky sexual behavior.
Data analysis
RESULTS
Socio-demographic characteristics
| Variable | Frequency | Percentage |
| Grade Level | ||
| 11th | 252 | 53.3 |
| 12th | 221 | 46.7 |
| Sex | ||
| Male | 274 | 57.9 |
| Female | 199 | 42.1 |
| Age | ||
| 16-19 | 369 | 78.2 |
| >= 20 | 104 | 21.8 |
| Marital Status | ||
| Single | 440 | 93 |
| Married | 18 | 3.8 |
| Living together before marriage | 15 | 3.2 |
| Religion | ||
| Orthodox | 272 | 57.5 |
| Muslim | 71 | 15 |
| Protestant | 110 | 23.3 |
| Catholic | 12 | 2.5 |
| Others | 8 | 1.7 |
| Living Arrangement | ||
| Living with parents | 288 | 60.9 |
| Living away from parents | 185 | 39.1 |
| Attend Religious Program | ||
| Yes | 342 | 72.3 |
| No | 131 | 27.7 |
| Frequency of Attending Religious Program/Week | ||
| 1 to 3 days per week | 220 | 64.3 |
| 4 to 7 days per week | 122 | 35.7 |
| Month Family Income | ||
| 400-900 | 176 | 37.2 |
| 901-1500 | 148 | 31.3 |
| > 1501 | 149 | 31.5 |
Risky sexual behaviors
| Variable | Frequency | Percent |
| Had ever had sexual intercourse | ||
| Yes | 188 | 39.7 |
| No | 285 | 60.3 |
| Sex =188 | ||
| Male | 122 | 64.9 |
| Female | 66 | 35.1 |
| Age at first sex n=188 | ||
| 14175 | ||
| >=18 years | 47 | 25 |
| Sexual partner n=188 | ||
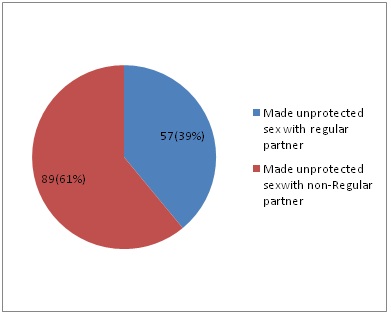
| Regular partner /friend | 89 | 47.3 |
| Non regular partner | 99 | 52.7 |
| Use condom during the 1st sexual intercourse n=188 | ||
| Yes | 83 | 44.1 |
| No | 105 | 55.9 |
| Condom use consistently n=83 | ||
| Yes | 38 | 45.8 |
| No | 45 | 54.2 |
| Having more than one sexual partner in the last six months | ||
| Yes | 96 | 51 |
| No | 92 | 49 |
| Make unprotected sexual intercourse in the last six months | ||
| No | 42 | 22.3 |
| Yes | 146 | 77.7 |
| Ever had sex with CSW | ||
| Yes | 15 | 8 |
| No | 173 | 92 |
| Number of sexual partner since start sex | ||
| One | 117 | 62.2 |
| Two and above | 71 | 37.8 |
Substance use practices and other related behavior
| Variable | Frequency | Percent |
| Ever go to night club | ||
| Yes | 68 | 14.4 |
| No | 405 | 85.6 |
| Frequency Per Month n=68 | ||
| 1 to 3 days/month | 60 | 88.2 |
| 4 and above days /month | 8 | 11.8 |
| Watch Pornography | ||
| Yes | 153 | 32.3 |
| No | 320 | 67.7 |
| Ever use alcohol in the last six months | ||
| Yes | 133 | 28.1 |
| No | 340 | 71.9 |
| Frequency Per Month | ||
| Always | 6 | 4.5 |
| Occasionally | 127 | 95.5 |
| Use Khat | ||
| Yes | 54 | 11.4 |
| No | 419 | 88.6 |
| Frequency Per Month | ||
| Always | 7 | 13 |
| Occasionally | 47 | 87 |
| Ever use Shisha/Hashish | ||
| Yes | 17 | 3.6 |
| No | 457 | 96.4 |
| Substance Use | ||
| Yes | 68 | 14.4 |
| No | 405 | 85.6 |
| Make sex after use addictive substances n=68 | ||
| Yes | 49 | 72 |
| No | 19 | 18 |
| After which substance use make sex | ||
| Alcohol | 37 | 75.6 |
| Khat | 9 | 18.4 |
| Shisha | 2 | 4 |
| Cigarette | 1 | 2 |
| Ever got VCT service | ||
| Yes | 139 | 29.4 |
| No | 334 | 70.6 |
Attitudes towards HIV/AIDS
| Variable | Frequency | Percent |
| All human beings are vulnerable to HIV | ||
| Strongly agree | 64 | 13.5 |
| Agree | 134 | 28.3 |
| Disagree | 182 | 38.5 |
| Strongly disagree | 77 | 16.5 |
| I do not know | 16 | 3.4 |
| Adolescents are highly risk for HIV | ||
| Strongly agree | 168 | 35.5 |
| Agree | 170 | 35.9 |
| Disagree | 88 | 18.6 |
| Strongly disagree | 37 | 7.8 |
| I do not know | 10 | 2.1 |
| You are vulnerable to HIV | ||
| Strongly agree | 22 | 4.7 |
| Agree | 64 | 13.5 |
| Disagree | 207 | 43.8 |
| Strongly disagree | 170 | 35.9 |
| I do not know | 10 | 2.1 |
Factors associated with risky sexual behaviors
| Variable | Risk Behavior | COR, 95%CI | AOR, 95% CI | |
| No | Yes | |||
| Sex | ||||
| Male | 193 | 81 | 1.8 (1.147,2.76)* | 0.79 (0.40 ,1.56) |
| Female | 161 | 38 | 1 | 1 |
| Age | ||||
| 16-19 | 284 | 85 | 1 | 1 |
| > 20 | 69 | 34 | 1.7 (1.02,2.65)* | 1.14 (0.56,2.28) |
| Living Arrangement | ||||
| With family | 253 | 35 | 1 | 1 |
| Away from family | 101 | 84 | 6.0 (3.81,9.49)* | 3.6 (1.84,6.89)* |
| Attend Religious Programs | ||||
| Yes | 295 | 47 | 1 | 1 |
| No | 59 | 72 | 7.7 (4.83,12.16)* | 4.1 (2.03,8.11)* |
| Drinking alcohol in the last 6 months | ||||
| No | 307 | 33 | 1 | 1 |
| Yes | 47 | 86 | 17 (10.27,28.21) | 6.9 (3.35,14.35)* |
| Show pornography in the last 6 month | ||||
| No | 297 | 23 | 1 | 1 |
| Yes | 57 | 96 | 21.8(12.72,37.17* | 7.2(3.67, 14.17)* |
| Chaw Khat | ||||
| No | 38 | 81 | 1 | 1 |
| Yes | 16 | 38 | 9.9 (5.27, 18.65)* | 1.5 (0.60, 3.79) |
| Family Income | ||||
| 400-900 birr | 114 | 62 | 2.16 (1.30,3.58)* | 2.6 (1.24,5.59)* |
| 901-1500 birr | 121 | 27 | 0.89 (0.49,1.58) | 0.86 (0.38,1.99) |
| >1500 birr | 119 | 30 | 1 | |
DISCUSSION
This finding indicated that the overall risky sexual behaviors were found to be 25.2%. This result is higher compared to study done in Boditi, Humera and Benishangul which showed that the prevalence of risky behaviors were 17.9%, 13.7% and 19.8% respectively [13-15]. This disparity might be due to the difference on study period. The attention that was given towards HIV prevention and controlling activities is seemed to be decreased in Ethiopia due to unexplained reasons.
This study also presented that being males behaved more risky sexual behavior than female students (68.1% male Vs 31.9% female) and this result is similar to study done in Humera, which showed risky sexual behaviors were predominantly practiced among male students (93.1% male Vs 6.9% female) [14]. This may indicated that male adolescents/youth practicing risky sexual behavior could be as a result of substance use and its consequences. About 96 (51%) of the study participants who had ever practiced sex had more than one sexual partner in the last 6 months. This finding is higher than study finding of Boditi and Benishangul in which 8.7% and 35.1% was reported having more than one sexual partner in the last 6 months, respectively [13,15].
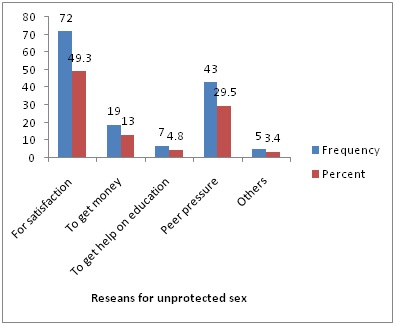
In this study 15 (8%) of the study participants who had ever practiced sexual intercourse had practiced sex with commercial sex workers and this is comparatively higher than the study finding from Benishangul that revealed 5.5% [15]. The major reasons reported for practicing unprotected sexual intercourse encounter in those who ever practiced sexual intercourse 72 (49.3%) of them to get satisfaction and 43 (29.5%) of the respondents was due to peer pressure. Similarly, studies conducted in Benshangul and Boditi showed that sexual desire and peer pressure were among the motivators with risky sexual behaviors [13,15].
This study found that personal perception about vulnerability to HIV, 207 (43.8%) and 17 (35.9%) of respondents disagreed and strongly disagreed as they are vulnerable to HIV, respectively. This is in line with the study conducted from Benshangul it revealed that only 24.5% of students perceived that they were at risk to HIV infection, 12.7 % did not know whether they are at risk or not and 62.9% they are perceived not at risk [15]. Low level of risk perception in this study might suggest school youth do not sense the consequence of risky sexual behavior which needs intensive intervention in developing life skills of youth.
The study revealed that risky sexual behavior was significantly associated with living arrangement of the students. Students who were living away from their parent were 3.6 times more vulnerable to risky sexual behavior than living with their parents (AOR=3.6, 95% CI 1.84-6.89). This is in lines with the study’s findings of Boditi, Jimma and Humera which revealed that students living away from their parents were more likely to practice risky sexual behavior than students who living with their parents [12-14]. This was supported by the FGD and they described the scenario as follows “female students who lived away from parents rented in the town are commonly make a relationship with ‘Suger Dady’ work in the town, so they are vulnerable to sex related problem and their consequences.”
In this study strong association between not attending religious program and risky sexual behavior were observed. Those who did not attend religious programs were 4.1 times more exposed to risky sexual behavior than those who attended religious programs (AOR=4.1 95% CI. 2.03-8.11). This study finding was in line with study done in Humera which elaborated not participating in any religious programs [AOR=6.17, 95% CI. 2.24-17.16] were the factors that increase the odds of practicing risky sexual behavior and Jimma Zone preparatory schools which showed that those who did not visit religious were 6 times risky compare than their counterparts [12,14].
Drinking alcohol was also significantly associated with risky sexual behaviors. That is, those who drink alcohol were 6.9 times risk to practice risky sexual behavior when compared to those who did not drink alcohol in the last 6 months (AOR=6.9, 95% CI. 3.35-14.35). This study was in agreement with study findings of Jimma, Benishangul and Brazil, which strengthens the association between drinking alcohol and risky behavior [12,15,16]. This is supported by the qualitative findings, that is one of the participants described the scenario as follows “students who are addicted by different substance including alcohol are at high risk for HIV/AIDs, since they will not consciously make unprotected sex or they do not consistently use condom.”
Similarly, those who watch pornography were 7.2 times more at risk for risky sexual behavior than those who did not watch pornography (AOR=7.2, 95% CI. 3.67-14.17). This study was consistent with study done in Humera [14] which explained that not exposed to pornographic movie is a factor that prevent [AOR=0.36, 95%CI: 0.32-0.91] the odds of practicing risky sexual behavior among the students. This is supported by the qualitative findings, that is one of the participants described the scenario as follows “nowadays majority youth are involved to sexual experimentation being pushed by impulse due to watch sex imitative films or pornography.”
Moreover, monthly family income less than 900 birr were 2.6 times more vulnerable to practice risky sexual behavior than those their family income is greater than 1500 birr (AOR=2.6 95% CI. 1.24-5.59). This study is consistent with study done in Hawassa, which reveals that girls who were with low economical status, more likely to had sexual relation with sugar daddies than their counterparts [17]. This is supported by the qualitative findings, that is one of the participants described “student who live away from their parents or live rented from less economic status are mainly influenced to make sexual intercourse with sugar daddies /merchants live in the town for the purpose of money ”
The study used both qualitative and quantities data as strong side. On the other hand, the study design was cross-sectional, which implies that the direction of causal relationships cannot always be determined. Moreover, since the issue of sex and related issue are sensitive, the study participants might be biased.
CONCLUSION
Considerable proportions of the students were practicing risky sexual behaviors. Not living with family, exposed to pornographic movies, not attending religious programs, drinking alcohol and low family income were the factors that increase the likelihood of practicing risky sexual behavior in the study participants.
RECOMMENDATION
Based on the above findings this study recommends that the Mizan Tepi University HIV/AIDs mainstreaming, school administration and health office of the three zones should take the initiative to bring about healthy sexual behaviors among their school youths by establishing and strengthening anti-AIDS and reproductive health clubs in the schools.
DECLARATIONS
Ethics approval and consent to participate
FUNDING
The research was funded by Mizan Tepi University.
AUTHORS' CONTRIBUTIONS
TK involved in the study design, data collection and analysis. AJ involved in the study design, data collection and analysis and drafted the manuscript. KM involved in study design, data collection and analysis. All authors read and approved the final manuscript.
ACKNOWLEDGEMENT
We thank to Mizan Tepi University for the financial support of the study. We also acknowledge the priceless support given by all who participated in the study, especially the study participants and data collectors.
REFERENCES
- OSSREA (2006) The HIV/AIDS Challenge in Africa: An Impact and Response Assessment: Executive Summaries of Findings of Research Projects Carried Out in Ethiopia, Kenya, South Africa, and Zimbabwe. OSSREA, Addis Ababa, Ethiopia Pg no: 101.
- Tadesse M, Daniel A (2010) Gender Mainstreaming Experiences from Eastern and Southern Africa. African Books Collective, Oxford, England, UK, Pg no: 173.
- Ahmed FA, Moussa KM, Petterson KO, Asamoah BO (2012) Assessing knowledge, attitude, and practice of emergency contraception: a cross- sectional study among Ethiopian undergraduate female students. BMC Public Health 12: 110.
- International Planned Parenthood Federation (IPPF) (1994) Understanding Adolescents, in An IPPF Report on Young People’s Sexual and Reproductive Health Needs. London, UK.
- EPHA (2003) Task force Adolescent Reproductive Health Global and National initiatives: Lesson Learned. EPHA, Belgium.
- Central Statistical Agency (2014) Ethiopia Mini Demographic and Health Survey 2014. Addis Ababa, Ethiopia
- Pharo H, Sim C, Graham M, Gross J, Hayne H (2011) Risky business: executive function, personality, and reckless behavior during adolescence and emerging adulthood. Behav Neurosci 125: 970-978.
- Prinstein MJ, La Greca AM (2004) Childhood peer rejection and aggression as predictors of adolescent girls' externalizing and health risk behaviors: a 6-year longitudinal study. J Consult Clin Psychol 72: 103-112.
- Russell TV, Do AN, Setik E, Sullivan PS, Rayle VD, et al. (2007) Sexual risk behaviors for HIV/AIDS in Chuuk State, Micronesia: the case for HIV prevention in vulnerable remote populations. PLoS One 2: 1283.
- James-Traore T, Magnani R, Murray N, Senderowitz J, Speizer I, et al. (2002) Internation strategies that work for youth: Summary of focus on young adults End of program report. North Carolina, USA.
- Scholl Ed, Schueller J, Gashaw M, Wagaw A, Michael LW (2004) Assessment of Youth Reproductive Health Programs in Ethiopia. USAID, Washington, D.C, USA.
- Fentahun N, Mamo A (2014) Risky sexual behaviors and associated factors among male and female students in Jimma zone preparatory schools, south west Ethiopia: comparative study. Ethiop J Health Sci 24: 59-68.
- Daka D, Shaweno D (2014) Magnitude of risky sexual behavior among high school adolescents in Ethiopia: A cross-sectional study. J Public health Epidemiol 6: 211-215.
- Dadi AF, Teklu FG (2014) Risky sexual behavior and associated factors among grade 9-12 students in Humera secondary school, western zone of Tigray, NW Ethiopia, 2014. J Public Health 2: 410-416.
- Agajie M, Belachew T, Tilahun T, Amentie M (2015) Risky Sexual Behavior and Associated Factors Among High School Youth in Pawe Woreda Benishangul Gumuz Region. J Clin Med 4: 67-75.
- Sanchez ZM, Martins SS, Opaleye ES, Moura YG, Locatelli DP, et al. (2011) Social factors associated to binge drinking: a cross-sectional survey among Brazilian students in private high schools. BMC Public Health 11: 201.
- Molla M, Mitiku L (2001) Transactional Sex with “Sugar Daddies” among Female Preparatory Students: HIV Risk Assessment in Hawassa Town, SNNPR, Ethiopia. Collage of Health Science, School of Public Health, Addis Ababa, Ethiopia.
Citation: Kahsay T, Jejaw A, Mulatu K (2017) Risky Sexual Behaviors and Associated Factors among Mizan, Bonga and Tepi Preparatory School Students, Southwestern, Ethiopia, 2016: A Cross Sectional Study. J AIDS Clin Res Sex Transm Dis 4: 013.
Copyright: © 2017 Tensay Kahsay, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.