Technology and Sexual Health in Adolescence: An Integrated Approach for STI and HIV Prevention
*Corresponding Author(s):
Zafra-Agea JADoctoral Programme In Health Sciences, University Of Seville, Spain
Email:jzafra@umanresa.cat
Abstract
This study aims to evaluate the effectiveness of a technology-based sexual health education program on knowledge and attitudes towards HIV and other STIs among second-cycle adolescents (aged 14-15). A quantitative, descriptive, and prospective study was conducted with an intervention group and a control group. Three longitudinal follow-up assessments were performed, including baseline, a fourth-month assessment during the intervention, and a nine-month follow-up post-intervention. The intervention involved a health blog as a supplementary component to the "Health and School" program, targeting knowledge and attitudes related to sexuality, sexually transmitted diseases, and affection. The study included 292 secondary school students divided into control (N=144) and intervention (N=148) groups. Assessments considered perceptions and behaviors related to knowledge about HIV and other STDs/STIs, attitudes towards HIV, health anxiety, and AIDS phobia. Statistical analysis revealed significant differences in health perception, knowledge about HIV transmission, and other STDs/STIs between the control and intervention groups. Early affective-sex education sessions positively impacted health perception and behaviors, reducing anxiety in adolescents. School nurses play a crucial role in promoting health, preventing sex-related diseases, and fostering healthy attitudes and relationships from a gender perspective.
Keywords
adolescents; affectivity-sexuality; gender; promotion; schools; STD/STI.
Introduction
Adolescence is universally recognized as a stage of transformation marked by significant changes in physical, psychological, social, and emotional domains, serving as a crucial bridge between childhood and adulthood. During this period, adolescents embark on an identity search that encompasses aspects such as self-acceptance, objective knowledge, personality formation, sexual identity, vocation, and personal ideology with associated values. The fluidity of self-esteem and self-concept during adolescence is influenced by a variety of factors including upbringing, environment, context, and individual capacities [1].
Sexuality, an inherent aspect of the human experience, develops uniquely at each stage of life, transcending mere anatomy to encompass affective dimensions such as emotions, experiences, and cultural influences. Inadequate knowledge in this area can lead to risky behaviors impacting health, resulting in consequences such as unwanted pregnancies, sexually transmitted infections (STIs), or sexual abuse [2].
STIs pose a significant challenge to global health, with over a million people ac-quiring an STI each day according to the World Health Organization (WHO) and other health organizations. Common STIs include HIV, syphilis, gonorrhea, chlamydia, and human papillomavirus (HPV). Young people are particularly susceptible to STIs due to risky behaviors, lack of comprehensive sexuality education, and, in some cases, limited access to sexual health services.
The presence of an STI can significantly impact the mental and social health of young people, including stigmatization, discrimination, and difficulties in interpersonal relationships. STIs often disproportionately affect young women, highlighting gen-der inequalities in access to information and sexual health services. Additionally, young people may face barriers in accessing sexual health services such as lack of confidentiality, shame, and limited resources.
Gender stereotypes continue to influence how adolescents experience and express their sexuality, with gender identified as a risk factor for STI acquisition [3]. The justification for this study is based on the significant incidence of HIV cases among young people, underscoring the urgency of addressing comprehensive affective-sexual education [4]. While the prevalence of HIV and other STIs is showing a downward trend in Catalonia and Europe, the persistence of cases among young people is concerning [5].
Therefore, this study is justified as a comprehensive measure to address this issue, providing affective-sexual education tailored to the needs and realities of adolescents. By better understanding young people's previous experiences related to sexuality and affectivity, as well as their beliefs and attitudes [6], we can design more effective and personalized interventions that promote healthy behaviors and reduce the risk of contracting STIs, including HIV.
By contextualizing the factors influencing young people's sexual behaviors and identifying areas for intervention, this study can significantly contribute to disease prevention, sexual health promotion, and the overall well-being of the adolescent population. Additionally, by considering the gender perspective in health perception and affective-sexual education, this study aims to address gender inequalities that may in-fluence young people's behaviors and sexual experiences.
In summary, this study aims to fill a crucial gap in understanding and addressing adolescent sexual health, with the goal of promoting healthy development and safe sexual relationships during this critical stage of life.
Moreover, in the current digital era, access to information on sexual health has greatly expanded thanks to information and communication technologies (ICTs), [7,8]. Young people increasingly use the Internet and social media to seek information on sexual health, access educational resources, and connect with online communities [9,10]. Therefore, this study also aims to explore the role of technologies in searching for and disseminating information on sexual health among adolescents, recognizing their potential to complement and strengthen traditional educational interventions [11,12]. The main aim of this study is to assess how a technology-based sexual health education program influences knowledge and attitudes towards HIV and other STIs among second-cycle adolescents (aged 14-15).
Methods
Design: A quantitative, descriptive, and prospective study was conducted, involving both an intervention group and a control group. Three longitudinal follow-up assessments were carried out throughout the school year, including a baseline control, a fourth-month assessment during the intervention period, and a nine-month follow-up post-intervention.
Participants: The sample consisted of 292 students aged 14 to 15, enrolled in the third year of Compulsory Secondary Education (ESO), selected from two public secondary schools in the metropolitan area of Baix Llobregat in Barcelona (Spain). Of these, 124 were female and 168 were male, distributed into a control group of 144 students and an intervention group of 148.
Both schools, located in the same municipality, had a designated school nurse in health and had implemented the "Salut i Escola 2.0" program on their virtual classroom platform.
The program was specifically designed to improve knowledge and awareness of Sexually Transmitted Infections (STIs), including HIV/AIDS, due to the detection of cases in the young population. There was an identified urgent need to address this is-sue and provide teenagers with accurate and relevant information on how to prevent and protect themselves against these diseases. Therefore, the program interventions focused on educating students about the risks associated with STIs, safe sexual practices, and the importance of contraceptive methods. Additionally, stigmas and prejudices associated with STIs were addressed, aiming to promote a more comprehensive understanding and inclusive attitude towards these issues in the student community.
The intervention group, consisting of students from one of the secondary education institutes (IES), participated in six detailed sessions throughout the academic year on sexuality, affectivity, and Sexually Transmitted Infections (STIs), with the support of the "Salut i Escola 2.0" blog accessible from personal devices.
On the other hand, the control group, composed of students from another secondary school, did not receive specific interventions, but they were introduced to the blog for familiarization purposes, and questionnaires were distributed to them. This blog was integrated into the secondary school's website where everyone could access it.
The hypothesis was that classroom interventions, along with access to the blog as a technological tool, would enhance knowledge about sexuality and contraceptive methods, as well as perception of the risk of sexually transmitted diseases and unwanted pregnancies, promoting optimal sexual health conditions.
The intervention sessions were conducted every two weeks during school hours, led by a school nurse with training in affectivity and sexuality, and focused on education about STIs, safe sexual practices, and contraceptive methods. These sessions were supplemented with additional information on the blog, accessible from the institute's online platform, thus providing a reliable and easily accessible resource for students.
Measures
HIV/Aids knowledge scale for adolescents. It consists of 10 items with two response options (true or false). The total score ranges from 0 to 10. The scale has a three-factor structure: Risk behaviors, with an internal consistency of 0.78. Effects of HIV, with an internal consistency of 0.57. Transmission, with an internal consistency of 0.61. The reliability coefficient for the total scale will be 0.70 [13].
Attitudes towards HIV/AIDS scale for adolescents [14]. It consists of 12 items with four response alternatives (from 1 = strongly disagree to 4 = strongly agree). The questionnaire has an internal consistency of 0.77, and the items are grouped into four sub-scales: barriers (three items), screening tests (two items), condom use (four items) and affected persons (three items). The test-retest reliability for the total scale was 0.60 [15]. It includes 4 factors and total score (sum of all items). Attitude towards condom use when there are obstacles to its use: items 1, 2, 3. Attitude towards HIV testing: 4, 5. Attitude towards condoms: 6, 7, 8, attitude towards people living with HIV/AIDS: 10 (reversed), 11, 12 (reversed).
Health anxiety. This is a self-report that assesses concern about health, concern about bodily sensations and fear of the negative consequences of suffering from an ill-ness. It consists of 18 items with four response options that score 0 (no symptoms), 1 (mild symptoms), 2 (severe symptoms) or 3 (very severe symptoms). The internal consistency is 0.95 and the test-retest correlation ranges between 0.83 and 0.87. Shai has demonstrated good psychometric properties with both clinical and non-clinical populations. 2 factors and total score (sum of all items): fear of becoming ill from item 1 to 14, negative consequences of having an illness from item 15 to 18 [16].
Phobia on the AIDS Phobia Scale. The test assesses AIDS phobia, looking at the main dimensions of the disorder. It consists of 20 items with a 6-point Likert-type response scale (from 0 = strongly disagree to 5 = strongly agree). The scale has a bifactor structure: fear of infection (Cronbach’s alpha = 0.73) and fear of others/avoidance (Cronbach’s alpha = 0.70). Temporal stability after one week was 0.64. The higher the score, the higher the AIDS phobia. 2 factors and total score (sum of all items): Fear of infection and Fear of others/avoidance [17].
- Sampling and Statistical Analysis
Data Collection: All students from both high schools (292 students aged 14-15 years) were invited to participate. The questionnaires were administered by the principal investigator of the study with the assistance of the teaching staff. This process took place two days after the sessions and subsequently at 4 and 9 months after the intervention once the following academic year had commenced.
Data Analysis: Variables were described for both the overall sample and subgroups based on the condition (intervention vs. control group). Median and interquartile interval (first and third quartile) were used for quantitative variables, while absolute and relative frequencies were employed for categorical variables. Bivariate analysis utilized the Wilcoxon test, assuming a significance level of p=0.05.
Comparisons between the control and intervention groups were conducted longitudinally at three time points: baseline, month 4, and month 9. Effect size scores were calculated at month 4 and month 9, relative to the baseline score, with an effect size of 0.2 considered small, 0.5 moderate, and 0.8 large (Cohen, Cohen, West, & Aiken, 1988; Kazis, Anderson, & Meenan, 1989). Statistical processing of the data was carried out using the Project R for Statistical Informatics software.
Ethical Statement: The study adhered to the core principles of the Declaration of Helsinki and its subsequent revisions, as well as the standards of Good Clinical Practice. The study protocol received approval from the Ethics Committee of IDIAP Jordi Gol of Barcelona under the number P17/119. The protocol ensures the confidentiality of subjects' data in compliance with the provisions of the Organic Law on the Protection of Personal Data (15/1999 of December 13, LOPD).
Results
Of the 292 participants, 75% were 14 years old at the time of the pre-intervention questionnaire at baseline. Of the 292 participants, 75% were 14 years old at the time of the pre-intervention baseline questionnaire. 94.83% of the students were born in the province of Barcelona.
Regarding the adolescents' perception of health, 53% of the girls have a very good perception of health and 45% have a good perception of health. Eighty-two percent of boys have a good overall perception of health and only 11% perceive it as very good.
In Table1, significant gender-based differences were observed, with women exhibiting higher knowledge about other STIs, more positive attitudes toward condom use, HIV testing, and condoms, while no significant differences were found in general HIV knowledge, condom knowledge, HIV prevention knowledge, health anxiety, or AIDS-related fear between men and women.
|
|
Men (n=124) |
Women (n=168) |
p-valor |
|
Scale of Knowledge about HIV and other STIs |
|||
|
HIV Transmission Knowledge |
3.87 [2.54, 5.45] |
3.87 [2.82, 5.44] |
0.671 |
|
Other STIs Knowledge |
0.00 [0.00, 1.75] |
0.00 [0.00, 0.00] |
0.016 |
|
General HIV Knowledge |
4.39 [3.71, 5.53] |
4.18 [3.34, 5.52] |
0.202 |
|
Condom Knowledge |
4.88 [3.76, 5.81] |
5.12 [3.87, 5.89] |
0.357 |
|
HIV Prevention Knowledge |
4.14 [3.13, 5.60] |
4.45 [3.21, 5.62] |
0.258 |
|
Attitudes towards HIV |
|||
|
Attitude towards condom use when facing obstacles |
54.82 [41.79, 66.67] |
66.67 [51.82, 80.41] |
<0.001 |
|
Attitude towards HIV testing |
66.67 [66.67, 85.26] |
68.59 [66.67, 85.26] |
0.047 |
|
Attitude towards condoms |
66.67 [51.83, 73.99] |
67.96 [58.98, 82.04] |
0.004 |
|
Attitude towards people living with HIV/AIDS |
44.97 [33.33, 54.12] |
43.75 [33.33, 55.43] |
0.209 |
|
Health Anxiety |
|
|
|
|
Fear of getting sick |
27.72 [21.41, 35.08] |
29.45 [21.44, 39.48] |
0.373 |
|
Negative consequences of having a disease |
20.01 [6.99, 31.30] |
20.96 [9.46, 36.54] |
0.339 |
|
AIDS-related Fear |
|||
|
Fear of infection |
17.59 [10.33, 24.65] |
18.36 [10.75, 25.87] |
0.631 |
|
Fear of others/avoidance |
72.65 [64.96, 78.17] |
71.90 [63.40, 79.39] |
0.665 |
Table 1: Scores on different scales related to HIV and STIs, by gender.
No significant differences were found in the scores on various scales according to the participants' age. These observations provide insights into the homogeneity in knowledge, attitudes, and anxieties related to HIV and STIs across different age groups.
Table 2 presents scores across various scales related to HIV and STIs, categorized based on whether participants sought information about sexuality on the internet. The findings indicate that individuals who consulted information online demonstrated significantly higher knowledge regarding HIV transmission compared to those who did not (p-value = 0.037). However, no significant differences were observed in knowledge about other STIs (p-value = 0.635), general HIV knowledge (p-value = 0.355), condom knowledge (p-value = 0.782), and HIV prevention knowledge (p-value = 0.176) between the two groups. Regarding attitudes towards HIV, no significant differences were found in attitudes towards condoms in challenging situations (p-value = 0.382), HIV testing (p-value = 0.609), condoms in general (p-value = 0.349), and towards people living with HIV/AIDS (p-value = 0.460). Similarly, there were no significant differences in health anxiety, including the fear of getting sick (p-value = 0.164) and the negative consequences of having a disease (p-value = 0.269). The analysis also revealed no significant disparities in AIDS-related fears, encompassing fear of infection (p-value = 0.107) and fear of others/avoidance (p-value = 0.190).
|
Knowledge about HIV and other ITS |
|
|
|
|
HIV Transmission Knowledge |
|||
|
Knowledge of Other STIs |
3.89 [2.87, 6.46] |
3.84 [2.56, 4.81] |
0.037 |
|
General HIV Knowledge |
0.00 [0.00, 0.00] |
0.00 [0.00, 0.00] |
0.635 |
|
Condom Knowledge |
4.27 [3.34, 5.94] |
4.25 [3.48, 5.27] |
0.355 |
|
HIV Prevention Knowledge |
5.12 [3.76, 5.96] |
5.07 [3.86, 5.83] |
0.782 |
|
Attitudes towards HIV |
4.43 [3.19, 5.96] |
4.19 [3.16, 5.43] |
0.176 |
|
Attitude towards Condoms in Challenging Situations |
|||
|
Attitude towards HIV Testing |
66.67 [44.08, 77.69] |
56.87 [44.08, 74.41] |
0.382 |
|
Attitude towards Condoms |
66.67 [66.67, 85.26] |
66.67 [66.67, 85.26] |
0.609 |
|
Attitude towards People Living with HIV/AIDS |
66.67 [59.16, 76.04] |
66.67 [54.60, 80.60] |
0.349 |
|
Health Anxiety |
44.97 [33.33, 55.03] |
42.19 [33.33, 55.03] |
0.460 |
|
Fear of Getting Sick |
|
|
|
|
Negative Consequences of Having a Disease |
27.67 [20.20, 34.98] |
28.90 [21.89, 38.70] |
0.164 |
|
AIDS-related Fear |
19.29 [8.84, 32.79] |
23.14 [9.46, 35.99] |
0.269 |
|
Fear of Infection |
|||
|
Fear of Others/Avoidance |
16.11 [9.27, 22.79] |
18.50 [11.16, 26.08] |
0.107 |
|
|
72.83 [66.95, 79.59] |
71.66 [62.74, 78.84] |
0.190 |
Table 2: Scores on Various Scales Regarding HIV and STIs, According to Seeking Information on Sexuality on the Internet.
These results suggest that seeking information on sexuality online may contribute to enhanced knowledge about HIV transmission, while other aspects of knowledge, attitudes, and anxieties show comparable patterns irrespective of online information seeking behavior.
The baseline scores (Table 3) for the intervention group reveal statistically significant differences in terms of knowledge. The table presents the median and interquartile range (1st and 3rd quartile) for each scale within the overall sample and across subgroups based on the intervention group. Additionally, the p-value from the Wilcoxon test is provided, with a significance level of p
|
|
Global Median [1stQ, 3rd Q] |
Control Group (n=144) |
Intervention group (n=148) |
p-value |
|
Knowledge scale on HIV and other STD/STI |
|
|
|
|
|
Knowledge HIV transmission |
3.87 [2.64, 5.44] |
3.80 [2.54, 4.29] |
4.16 [2.97, 6.44] |
<0.001 |
|
Knowledge of other STIs |
0.00 [0.00, 0.00] |
0.00 [0.00, 0.00] |
0.00 [0.00, 1.75] |
0.069 |
|
General HIV knowledge |
4.26 [3.38, 5.52] |
4.46 [3.85, 5.43] |
4.19 [3.27, 5.69] |
0.144 |
|
Condom knowledge |
5.08 [3.84, 5.84] |
5.14 [4.41, 5.84] |
4.88 [3.36, 5.89] |
0.031 |
|
HIV prevention knowledge |
4.19 [3.16, 5.62] |
4.14 [3.19, 5.31] |
4.70 [2.96, 5.98] |
0.024 |
|
Attitudes towards HIV |
|
|
|
|
|
Attitude towards condom use when barriers exist |
59.87 [44.08, 77.41] |
56.87 [44.08, 74.41] |
64.61 [42.02, 78.75] |
0.503 |
|
Attitude towards HIV testing |
66.67 [66.67, 85.26] |
66.67 [66.67, 81.41] |
70.52 [66.67, 85.26] |
0.196 |
|
Attitude towards condoms |
66.67 [56.03, 77.48] |
73.28 [59.34, 82.76] |
64.51 [52.37, 73.99] |
<0.001 |
|
Attitude towards people living with HIV/AIDS |
43.75 [33.33, 55.03] |
44.97 [33.33, 57.81] |
42.97 [33.33, 55.03] |
0.425 |
|
Health anxiety |
|
|
|
|
|
Fear of getting sick |
28.57 [21.42, 37.69] |
28.90 [20.17, 38.48] |
28.07 [21.67, 36.99] |
0.819 |
|
Negative consequences of having a disease |
20.67 [9.46, 34.39] |
17.18 [6.70, 32.79] |
23.29 [13.68, 35.99] |
0.030 |
|
AIDS Phobia |
|
|
|
|
|
Fear of infection |
18.07 [10.64, 25.43] |
19.86 [12.18, 29.27] |
15.39 [9.05, 21.32] |
<0.001 |
|
Fear of others/avoidance |
72.17 [63.75, 79.00] |
71.35 [60.23, 78.11] |
72.88 [66.95, 79.70] |
0.047 |
Table 3: Basal scores on the different scales on HIV and STDs, in the overall sample and according to intervention group.
This table presents the effect size at Month 4 and Month 9 for each scale in the control and intervention groups. Positive values indicate an increase, while negative values indicate a decrease.
Table 4 and Figure 1, presents the effect size at Month 4 and Month 9 for each scale in the control and intervention groups. Positive values indicate an increase, while negative values indicate a decrease.
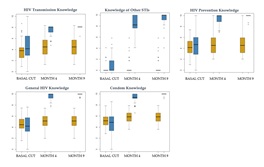 Figure 1: Evolution of scores in the subscales of the HIV and other STIs Knowledge Scale, according to the intervention group.
Figure 1: Evolution of scores in the subscales of the HIV and other STIs Knowledge Scale, according to the intervention group.
|
|
A Month 4 |
A Month 9 |
||
|
|
Control |
Intervention |
Control |
Intervention |
|
Knowledge Scale on HIV and Other STDs |
||||
|
Knowledge of HIV Transmission |
0.551 |
1.348 |
0.551 |
1.482 |
|
Knowledge of Other STDs |
0.141 |
7.356 |
0.141 |
8.315 |
|
General HIV Knowledge |
0.546 |
3.01 |
0.546 |
3.211 |
|
Condom Knowledge |
0.617 |
2.538 |
0.617 |
2.843 |
|
HIV Prevention Knowledge |
0.402 |
2.211 |
0.402 |
2.414 |
|
Attitudes Toward HIV |
||||
|
Attitude Toward Condom Use When Barriers Exist |
-0.024 |
0.661 |
-0.06 |
0.961 |
|
Attitude Toward HIV Testing |
-0.012 |
0.587 |
-0.117 |
0.653 |
|
Attitude Toward Condoms |
-0.097 |
0.605 |
-0.235 |
1.077 |
|
Attitude Toward People Living with HIV/AIDS |
0.123 |
0.754 |
0.12 |
1.283 |
|
Health Anxiety |
|
|
|
|
|
Fear of Getting Sick |
-0.282 |
0.178 |
-0.282 |
0.062 |
|
Negative Consequences of Having a Disease |
-0.081 |
0.035 |
-0.081 |
-0.463 |
|
AIDS Phobia |
||||
|
Fear of Infection |
0.025 |
-0.434 |
0.067 |
-0.149 |
|
Fear of Others/Avoidance |
0.189 |
-2.149 |
0.492 |
-3.077 |
Table 4. Effect Size at Month 4 and Month 9 by Intervention Group on Various Scales Related to HIV and STDs.
In terms of knowledge, a statistically significant increase is observed in HIV transmission in the intervention group at both time points, with effect sizes of 1.348 and 1.482, respectively, compared to the control group. The knowledge scale of other STIs shows a particularly notable impact in the intervention group at both periods, with effect sizes of 7.356 and 8.315 at Months 4 and 9, respectively. However, no statistically significant differences are observed in general HIV knowledge between the two groups. Regarding attitudes towards HIV, the intervention group experiences a statistically significant improvement in the attitude towards condom use in challenging situations, with effect sizes of 0.661 at Month 4 and 0.961 at Month 9. Additionally, a statistically significant decrease is observed in fear of others or avoidance in the intervention group, with effect sizes of -2.149 and -3.077 at Months 4 and 9, respectively. These findings suggest statistically significant and sustained impacts of the intervention on knowledge and attitudes related to HIV and STIs over time.
Discussion
Our research aligns with previous studies by demonstrating a positive impact on the affective-sexual health of adolescents in the intervention group. The incorporation of Information and Communication Technologies (ICTs), particularly through the use of a blog, emerges as a valuable tool for knowledge construction. Our findings support the notion that the blog serves as a dynamic platform to address current issues in affectivity and sexuality, providing a continuous and updated source of information accessible to adolescents.
The integration of ICTs within the educational environment, exemplified by the COMPAS Program, highlights the potential of these technologies to create repositories of health promotion materials. This not only enhances accessibility but also provides a cost-effective means of disseminating information. The use of technology, such as blogs, facilitates the process of autonomous learning, allowing adolescents to explore topics relevant to their daily lives, thus contributing to knowledge construction in an engaging manner.
Additionally, the study recognizes the importance of Internet use by adolescents and its implications for intervention planning at both the school and family levels. The potential risks associated with excessive use of social networks and the Internet underscore the importance of informed and targeted interventions.
The effectiveness of our study, evidenced by the COMPAS Program, is noteworthy, especially in short-term results related to increased knowledge about HIV, improved attitudes toward HIV, condom use, HIV testing, and enhanced intention to use condoms. These results reflect the consensus that implementing interventions is more beneficial than not doing so, emphasizing the positive impact on HIV prevention among young people.
Furthermore, our study acknowledges the moderating role of gender and sexual status in the intervention's effectiveness. Non-sexually active adolescents and women showed more favorable results, underscoring the importance of early interventions to reduce sexual risk. Gender differences observed, with women exhibiting a more positive attitude toward condom use, highlight the need for gender-specific approaches in sexual health promotion.
In post-intervention consultations, women demonstrated greater knowledge about HIV and exhibited more positive attitudes toward condom use and people living with HIV. These findings align with the Theory of Planned Action, emphasizing the im-portance of forming positive attitudes to influence behavior. The results support the active role of public health nurses and school nurses in detecting risk behaviors and implementing integrative preventive strategies to enhance health perception within a salutogenic model.
Despite limitations, such as potential biases in self-reported data, our findings underscore the positive impact of the intervention and the potential of ICTs in promoting affective-sexual health among adolescents. Future studies could consider expanding the sample and incorporating qualitative interventions that account for gen-der differences in risk and protective factors related to sexual behavior.
Conclusions
In summary, this study demonstrates the effectiveness of a technology-based affective-sexual education program in improving knowledge, attitudes, and perceptions regarding HIV and other STIs among adolescents. The integration of technological tools, such as a blog, into the educational environment provides a dynamic and accessible platform for addressing sensitive sexual health topics. The findings highlight the importance of considering gender and internet use when designing interventions to promote sexual health among young people, with significant implications for the development of public health policies and programs aimed at enhancing adolescent sexual health in both educational and community settings.
Furthermore, the research achieves its objectives by confirming the proposed hypothesis: the implementation of prevention and promotion interventions in classrooms, coupled with access to the "Health and School 2.0" blog as a supporting tool, enhances knowledge about sexuality and contraceptive methods. There is also an improvement in the perception of the risk of sexually transmitted diseases, health anxiety, and un-planned pregnancies, thereby optimizing the sexual health conditions of adolescents.
The "Health and School" blog emerges as an effective supporting tool for the pro-motion and prevention of risk behaviors related to sexuality in the school environment. It facilitates the transmission of information, skill development, and health education.
In a context where adolescents report earlier initiation of sexual activity and an increase in the number of sexual partners, the intervention proves to be crucial. The growing trend of the risk of contracting sexually transmitted infections reflects a lack of information and an unfavorable attitude toward the use of protective methods.
In conclusion, this research highlights the effectiveness of a health education intervention, implemented by nursing professionals, and integrated into high schools with the support of the blog. Accessibility, information endorsed by healthcare professionals, and contrasting information prove to be key elements in preventing risky sexual behaviors, sexually transmitted diseases, and promoting self-esteem among adolescents.
Author Contributions
José Antonio Zafra conceived the idea, designed the study, conducted the research and subsequent analysis, and drafted the manuscript. As the corresponding author, José Antonio Zafra holds the authority to grant a worldwide license.
Funding
This project did not receive any financial support.
Institutional Review Board Statement
The research protocol was approved by the Research Ethics Committee of IDIAP Jordi Gol: ref. no. P17/119.
Informed Consent Statement
All participants signed the consent form for their participation; in the case of dealing with minors, parents, guardians, or legal representatives provided the consent.
Data Availability Statement
The authors would be pleased to share a clean copy of the database; please contact the corresponding author for further details.
Acknowledgments
The authors express their gratitude to all the students, families, directors, and teachers of the two secondary schools in Baix Llobregat who participated in the study.
Conflicts of Interest
The authors declare no conflicts of interest in this study.
References
- Sanz-Martos S, López MIM, Álvarez GC, Álvarez NC (2019) Efectividad de Las Intervenciones Educativas Para La Prevención Del Embarazo En La Adolescencia. Atención Primaria 51: 424-434.
- Goldfarb ES, Lieberman LD (2021) Three Decades of Research: The Case for Comprehensive Sex Education. Journal of Adolescent Health 68: 13-27.
- Meherali S, Rahim KA, Campbell S, Lassi ZS (2021) Does Digital Literacy Empower Adolescent Girls in Low- and Mid-dle-Income Countries: A Systematic Review. Frontiers in Public Health 9: 761394.
- Saura S, Jorquera V, Rodríguez D, Mascort C, Castellà I, et al. (2019) Percepción Del Riesgo de Infecciones de Transmisión Sexual/VIH En Jóvenes Desde Una Perspectiva de Género. Atención Primaria 51: 61-70.
- CEEISCAT Centre d’Estudis Epidemiològics Sobre Les Infeccions de Transmissió Sexual i Sida de Catalunya (CEEISCAT) (2022) Vigilància Epidemiològica de Les Infeccions de Transmissió Sexual (ITS) a Catalunya Informe Annual. CEEISCAT, Spain.
- Guerrero Ramírez CI, Espadafor López B, Arias-Santiago S, Buendía-Eisman A (2023) Programa de Intervención Escolar Para La Prevención de Las Infecciones de Transmisión Sexual. Actas Dermosifiliogr 114: 90-91.
- Bozzola E, Spina G, Agostiniani R, Barni S, Russo R, et al. (2022) The Use of Social Media in Children and Adolescents: Scoping Review on the Potential Risks. Int J Environ Res Public Health 19: 9960.
- Kokka I, Mourikis I, Nicolaides NC, Darviri C, Chrousos GP, et al. (2021) Exploring the Effects of Problematic Internet Use on Adolescent Sleep: A Systematic Review. International Journal of Environmental Research and Public Health 18: 760.
- Lameiras FM, Martínez RR, Carrera FM V, Rodríguez CY (2021) Sex Education in the Spotlight: What Is Working? Systematic Review. Int. J. Environ. Res. Public Health, 18: 2555.
- Eppes EV, Augustyn M, Gross SM, Vernon P, Caulfield LE, et al. (2023) Engagement With and Acceptability of Digital Media Platforms for Use in Improving Health Behaviors Among Vulnerable Families: Systematic Review. J Med Internet Res 25: 40934.
- Lau PW, Lau EY, Wong DP, Ransdell LA (2011) Systematic Review of Information and Communication Technology–Based Interventions for Promoting Physical Activity Behavior Change in Children and Adolescents. J Med Internet Res 13: 48.
- Orte C, Sarrablo LR, Nevot CL (2022) Systematic Review on Affective-Sexual Education Programs and Inter-ventions for Adolescents. REICE 145-164.
- Espada JP, Guillén Riquelme A, Morales A, Orgilés M, Sierra JC (2014) Validation of an HIV and Other Sexually Transmitted Infections Knowledge Scale in an Adolescent Population. Atencion Primaria 46: 558-564.
- Carratalá E, Espada JP, Orgilés M (2013) Conocimientos y Actitudes Hacia El VIH/SIDA: Diferencias Entre Adolescentes Es-pañoles Con Padres Casados y Divorciados. Salud Mentl 36.
- Espada JP, Huedo Medina TB, Orgilés M, Secades R, Ballester R, et al. (2009) Psychometric Properties of the HIV/AIDS Knowledge Scale for Spanish Adolescents (HIV-KS). Heal Addict y Drog 9: 149-164.
- Abramowitz JS, Deacon BJ, Valentiner DP (2007) The Short Health Anxiety Inventory: Psychometric Properties and Construct Validity in a Non-Clinical Sample. Cognitive Therapy and Research 31: 871-883.
- Vallejo MP, Saavedra RA, Gómez LM, Morales A, Abello Luque D, et al. (2018) Adaptación, Fiabilidad y Validez de Una Versión Breve de La Multicomponent AIDS Phobia Scale (MAPS) En Adolescentes Colombianos. Rev Iberoam Psicol y Salud 9: 42-57.
- Tamarit A, Schoeps K, Peris HM, Montoya CI (2021) The Impact of Adolescent Internet Addiction on Sexual Online Victimization: The Mediating Effects of Sexting and Body Self-Esteem. Int J Environ Res Public Health 18: 4226.
- Pampati S, Johns MM, Szucs LE, Bishop MD, Mallory AB, (2021) Sexual and Gender Minority Youth and Sexual Health Education: A Systematic Mapping Review of the Literature. Journal of Adolescent Health 68: 1040-1052.
- McCabe EM, McDonald C, Connolly C, Lipman TH (2019) Factors Associated With School Nurses’ Self-Efficacy in Provision of Asthma Care and Performance of Asthma Management Behaviors. The Journal of School Nursing 37: 353-362.
- Corral GGDJ, García CMDL, Herrera PJM (2022) Asertividad Sexual Autoeficacia y Conductas Sexuales de Riesgo En Adolescentes: Una Revisión de Literatura. ACC CIETNA Rev la Esc Enfermería 9: 167-177.
- Morales A, Carratalá E, Orgilés M, Espada JP (2017) Un Estudio Preliminar De La Eficacia De Un Programa De Promoción De La Salud Sexual En Adolescentes Con Padres Divorciados. Heal Addict 17: 37-44.
- Bossonario PA, Ferreira MRL, Andrade RLDP, Sousa KDLD, Bonfim RO, et al. (2022) Factores de Riesgo de Infección Por VIH Entre Adolescentes y Jóvenes: Revisión Sistemática. Rev Lat Am Enfermagem, Brazil.
- Bonilla AE, Rivas RE, Pascual GI (2021) Mitos Del Amor Romántico En Adolescentes: Relación Con El Sexismo y Variables Procedentes de La Socialización. Education XX1 24: 441-464.
Citation: Zafra JAA (2024) Technology and Sexual Health in Adolescence: An Integrated Approach for STI and HIV Prevention. J AIDS Clin Res Sex Transm Dis 8: 037.
Copyright: © 2024 Zafra-Agea JA, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.