Willingness to Accept Keratorefractive Surgery and its Barriers among Myopes at Eye Foundation Hospital Group, Nigeria
*Corresponding Author(s):
Agu Obiajulu ChidubemConsultant Ophthalmic Surgeon, Skipper Eye-Q Eye Hospital, 2 Udoma Street, Asokoro, FCT, Abuja, Nigeria
Tel:2347039430326,
Email:agu.oc@yahoo.com
Abstract
Objectives: The objective of the study was to determine the willingness to accept keratorefractive surgical procedures and its barriers to uptake among myopes at Eye Foundation Hospital Group, Nigeria.
Materials & Methods: A descriptive, cross-sectional study was carried out at the Eye Foundation hospital group, involving consecutive consenting new patients diagnosed with any form of myopia. The research involved the administration of semi-structured questionnaires, in-depth interviews and focus group discussions, which were used to collect information on socio-demographic characteristics, willingness to accept the procedure and barriers to uptake of keratorefractive surgery.
Results: The study involved 302 participants who were enrolled, and their ages ranged from 18 years to 57 years old, with an average age of 30.48±8.44 years. Twenty-one per cent of the participants were willing to accept the surgery if offered, 45% of the participants were not willing to accept the procedure and 34% of the participants were not sure if there would accept it or not. Participants with high myopia (chi-square p<0.001) were more willing to accept keratorefractive surgery. Reasons for accepting to do surgery keratorefractive surgery were; tired of using spectacles/contacts (87.3%), career reason (11.1%), do not want to use spectacles (6.3%), beautification (6.3%) and leisure (1.6%). The reasons for not opting for keratorefractive surgery were; fear of damage (59.1%), lack of awareness (41.6%) and financial constraints (40.9%).
Conclusion: The willingness to accept keratorefractive surgical services in this study was low. The main barriers to the uptake of the services were fear of damage, lack of awareness and financial constraints and there is a need for patient education to improve surgical uptake.
Keywords
Willingness to accept; Fear of damage; Lack of awareness; Keratorefractive surgery; Myopia
Abbreviations
BCVA: Best Corrected Visual Acuity
CDVA: Corrected Distance Visual Acuity
D: Diopter
EFHG: Eye Foundation Hospital Group
LASIK: Laser Assisted In-situ Keratomileusis
LE: Left Eye
LASEK: Laser Assisted Sub Epithelial Keratomileusis
PRK: Photorefractive Keratectomy
PH: Pin Hole
RK: Radial Keratectomy
RE: Right Eye
SE: Spherical Equivalent
SMILE: Small Incision Lenticular Extraction
SIA: Surgically Induced Astigmatism
TIA: Target Induced Astigmatism
UCVA: Uncorrected Distance Visual Acuity
VA: Visual Acuity
WHO: World Health Organization
Research Highlights
- Recent studies in Nigeria have shown a steady rise in the prevalence of myopia
- Myopia is one of the leading causes of visual impairment and blindness worldwide
- The main barriers to the uptake of the services were fear of damage, lack of awareness and financial constraints
Introduction
Refractive error is the state of an eye in which light rays are not focused on the retina, resulting in a blurred image. They affect people without consideration for age, gender, or ethnicity but are strongly influenced by socioeconomic status, being both a cause and a consequence of poverty and limited access to ophthalmic care [1]. Blurred vision from refractive error can be treated in most cases by neutralizing the refractive error with corrective lenses, such as spectacles and contact lenses or by refractive surgery [1].
Myopia (nearsightedness) is a refractive error, in which images of distant objects focus in front of the retina when accommodation is relaxed. Recent studies in Nigeria have shown a steady rise in the prevalence of myopia [2,3]. Myopia and high myopia were estimated to affect 27% (1,893 million) and 2.8% (170 million) of the world population, respectively, in 2010, making myopia one of the leading causes of visual impairment and blindness worldwide, hence a major public health challenge [4].
Keratorefractive surgeries encompass surgical procedures used to improve the refractive state of the eye and decrease or eliminate dependency on corrective lenses.
It has been estimated from studies that 14% to 35% of prospective keratorefractive surgical patients ended up not having the surgery performed, as a result of low corneal thickness, suspicion of keratoconus, and a change of mind (due to financial constraints and fear) even after more information has been given during the preoperative examination [5,6].
Keratorefractive surgical services, being a relatively new field in a developing country like Nigeria, could be confronted with the challenge of low surgical uptake among prospective patients. Therefore, it is pertinent to know the willingness to accept the procedure and barriers to its uptake among myopes in a centre that readily offers this service to provide data for planning, improving surgical uptake and advocacy.
Methods
This descriptive prospective cross-sectional study was conducted at different locations of the Eye Foundation Hospital Group, Nigeria. This study followed the guidelines as contained in the Declaration of Helsinki and approval was obtained from the Ethics and Research Committee of the Lagos State University Teaching Hospital, Ikeja, Lagos, Nigeria. The participants were patients who came for eye consultations in the eye clinics of the health facility.
- Study design
The participants in this study were new consenting adult patients diagnosed with any form of myopia aged 18 years or older. Written consent was obtained after the study had been explained to each participant. This study had both quantitative and qualitative components. The quantitative component included a prospective study and the qualitative component included in-depth interviews and focused group discussions (FGD).
Participants were interviewed using pretested semi-structured questionnaires (adapted from previous studies) [7]. Interviewer-administered semi-structured questionnaires, in-depth interviews and focused group discussions were used to collect information on socio-demographic characteristics, willingness to accept the procedure and barriers to uptake of keratorefractive surgery [8,9].
- Data analysis
The data were collated, entered into, IBM Statistical Package for Social Sciences (IBM-SPSS) version 26 (IBM Corp: Armonk, NY USA) and analyzed. The Chi-square was used to test associations between parameters. These include associations between degree of myopia/demographic characteristics and willingness to accept keratorefractive surgery. The Shapiro-Wilk test was used to determine the normality of quantitative variables. Student's t-test and Wilcoxin sign ranked tests were used for the comparison of continuous variables depending on normality. The results are displayed using tables, pie charts, and bar charts. The associations of statistical significance were taken at P < 0.05.
Results
A total of 302 participants were enrolled in this study. One hundred and fifty-six (51.7%) were male and one hundred and forty-six (41.3%) were female, with a mean age of 30.48±8.44 (18 to 57) years.
- Willingness to accept keratorefractive surgeries
After the educational session on keratorefractive surgery have been done, the varying responses of the participants with respect to their willingness to accept keratorefractive surgeries are as shown in figure 1.
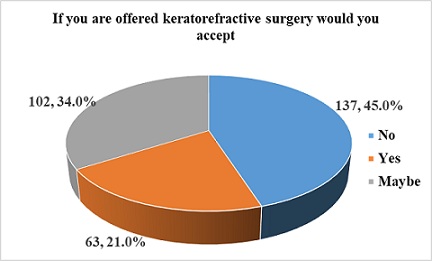 Figure 1: Willingness to accept keratorefractive surgery.
Figure 1: Willingness to accept keratorefractive surgery.
- Reasons for accepting to do keratorefractive surgery
Out of the 63 participants who were willing to undergo keratorefractive surgeries, 87.3% were tired of using spectacles/contacts while 11.1%, reported as career reasons, shown in table 1.
|
Reasons for accepting |
Frequency* N=63 |
Percentage (%) |
|
Tired of using spectacles/contacts |
55 |
87.3 |
|
Career reasons |
7 |
11.1 |
|
Do not want to use spectacles /contacts |
4 |
6.3 |
|
Beautification |
4 |
6.3 |
|
leisure |
1 |
1.6 |
|
No reason |
1 |
1.6 |
Table 1: Reasons for accepting to do keratorefractive surgery.
* Some participants gave multiple responses
- Barriers to uptake of Keratorefractive Surgery
Out of the 137 participants who were unwilling to undergo keratorefractive surgeries, 59.1% reported fear of surgery as their reason while 41.6%, reported as lack of awareness, shown in table 2.
|
Barriers |
Frequency* N=137 |
Percentage (%) |
|
Fear of surgery |
81 |
59.1 |
|
Lack of awareness |
57 |
41.6 |
|
Financial constraints |
56 |
40.9 |
|
Adverse effects |
27 |
19.7 |
|
Satisfied with vision |
9 |
6.6 |
|
Negative advice |
3 |
2.2 |
|
No reason |
3 |
2.2 |
Table 2: Barriers to uptake of keratorefractive Surgery.
* Some participants gave multiple responses
- Reasons for not being sure of accepting keratorefractive surgery
One hundred and two (34%) participants were not sure if they would have keratorefractive surgery or not. Reasons are shown in table 3.
|
|
Frequency* N=102 |
Percentage (%) |
|
Reasons for possible acceptance Tired of using spectacles/contacts |
60 |
58.8 |
|
Do not want to use spectacles /contacts |
28 |
27.4 |
|
Beautification |
8 |
7.8 |
|
Career reason |
2 |
2.0 |
|
No reason |
9 |
8.8 |
|
Reasons for possible non-acceptance
Financial constraint Fear of surgery Lack of awareness Adverse effects Satisfied with vision Negative advice No reason
|
62
51
36
20
1
2
3 |
60.8
50
35.5
19.6
1.7
3.3
5.0 |
Table 3: Reasons for not being sure of accepting keratorefractive surgery.
*Some participants gave multiple responses
- Willingness to accept keratorefractive surgery with associated variables
The results in table 4 showed the associations between willingness to accept keratorefractive surgeries and socio-demographic variables/degree of myopia. Degree of myopia showed significant association with willingness to accept keratorefractive surgery (chi-square p<0.001). However, there were no significant association between age, gender, place of residence, level of education, income, occupation and willingness to accept keratorefractive surgery.
|
Variable
|
willingness to accept keratorefractive surgery |
|||
|
|
Yes |
No |
Maybe |
p-value |
|
Age(years) <40 ≥40 |
57 (22.3) 6 (13.0) |
114 (44.5) 23 (50.0) |
85 (33.2) 17 (37.0) |
0.366 |
|
Gender Male Female |
36 (23.1) 27 (18.5) |
65 (39.7) 72 (49.3) |
55 (35.2) 47 (32.2) |
0.379 |
|
Place of residence Rural Urban |
8 (11.1) 55 (24.0) |
38 (52.8) 99 (43.0) |
26 (36.1) 76 (33.0) |
0.061 |
|
Level of education
≥Tertiary education |
7 (18.9) 56 (21.1) |
16 (43.3) 121 (45.7) |
14 (37.8) 88 (33.2) |
0.850 |
|
Occupation Unemployed Employed |
21 (19.3) 42 (21.7) |
55 (50.5) 82 (42.5) |
33 (30.2) 69 (35.8) |
0.406 |
|
Income (Annually/Naira) <1,000,000 ≥1,000,000 |
36 (20.1) 27 (22.0) |
81 (45.3) 56 (45.5) |
62 (34.6) 40 (32.5) |
0.898 |
|
Degree of myopia Low to moderate High myopia
|
31 (11.9) 32 (76.2)
|
133 (51.2) 4 (9.5)
|
96 (36.9) 6 (14.3)
|
<0.001* |
Table 4: Test of association between degree of myopia/demographic characteristics and willingness to accept keratorefractive surgery.
*Statistically significant
- Focused group discussion/in-depth interview
Fifteen (15) participants were enrolled in the focus group while twenty-one (21) participants participated in the in-depth interview. Barriers to the uptake of keratorefractive surgery and the motivation for uptake of keratorefractive surgery were the themes that emerged from the analysis.
- Barriers to uptake for keratorefractive surgery
The dominant barriers to the uptake of keratorefractive surgery were fear of complications and financial constraints. Many participants believed that the lack of awareness of the safety of the procedure in Nigeria and also the lack of trust in Nigerian doctors contributed greatly to the 'fear' seen in individuals.
Participant from focus group: 'Hmm…. Can't allow a doctor in Nigeria to touch my eye without seeing evidence of his/her success stories with previous patients'
Participant from focus group: 'My vision is good, I don't need it
Participant from an in-depth interview: 'Haaaaa…...where can I get such amount of money for the surgery? It's just for the financially privileged'
- Motivation for uptake of keratorefractive surgery
Three forms of motivation towards the uptake of keratorefractive surgery were tired of using spectacles, beautification and career reasons.
Most of the participants were tired of using spectacles and would do anything to make them stop wearing spectacles. The females generally reported that they were not able to show their make-up with their spectacles on and would love to be able to make up and move around without their spectacles.
Participant from an in-depth interview: 'I work as a customer care representative in a bank, I never liked it that I couldn't take out my spectacles and look like my other colleagues who do not wear spectacles. I felt they were more beautiful and smarter… now I have done the surgery, my self-worth is back. On the first day at work, my colleagues couldn't recognize me. They were amazed and said that I looked more beautiful'
Participants from the focus group: 'I have been using spectacles for 30 years and am tired. I want to be free from it'
Discussion
In this study, only 21% of the participants were willing to accept the surgery if offered while 34% of the participants were not sure if they would accept it or not, since they were just hearing it for the first time and would need assurance from evidence-based success stories from medical doctors, friends, colleagues or family members before accepting to do the procedure. This is similar to the findings of Ayanniyi et al. [10].
This study revealed a significant association between degree of myopia (chi-square p<0.001) and willingness to accept keratorefractive surgery. Participants with high myopia were more willing to accept keratorefractive surgery than those with mild to moderate myopia. This may be a reflection of the fact that the more myopia, the poorer the unaided vision and the more the need to depend on spectacles, henceforth, the drive to accept keratorefractive surgery. Concerning the focus group discussion and in-depth interview, keratorefractive surgery was mainly viewed as an innovative, risky, surgery for the financially privileged and needless since some patients may still need spectacles after the surgery while a few saw it as a welcome development if it would make them stop using spectacles. Participants indicated that ophthalmologists and other medical doctors rarely talk about the surgery during clinic visits with limited records of success rates in keratorefractive surgery in Nigeria and a lack of trust in the health system, thereby doubting the capacity of such surgery being done in Nigeria.
This may be due to the systemic failure of the Nigerian health sector with low annual budget allocation for capacity building and infrastructural development, leading to the underdevelopment of the general health facilities in the country and mistrust seen among individuals.
The reasons why participants opted for surgery in this study, were due to being tired of using spectacles and contact lenses (87.3%), career reasons (11.1%), not wanting to use spectacles and contacts (6.3%), beautification (6.3%) and leisure (1.6%). These were similar to the findings in previous studies.1,7,8,10 This may be a reflection of the fact that myopes require their spectacles/contacts almost all the time to navigate around their environs, increasing their dependence on them and contact lens wear requires good hygiene protocols at all times. This may become burdensome, increasing the tendency for sub-optimal spectacle/contact lens wear. Dependence is worst with high myopes, making them more likely to visit the refractive surgical clinics for possible surgery and this study revealed that 76.2% of participants with high myopia were willing to accept keratorefractive surgery, if offered. Dependence on spectacles/contacts may not also be suitable for some careers like the military, pilots, hostesses, models and those that engage in sports, thereby increasing the tendency to opt for keratorefractive surgery. Leisure is another important factor, some individuals may not want to engage in leisure activities like going to the beach and attending parties, wearing their spectacles/contacts lens. Females may also want to show their make-up while attending events and not all individuals are comfortable with wearing contacts.
This study revealed that 45% of the participants were not willing to accept the procedure. They cited fear of surgery (59.1%), lack of awareness (41.6%), financial constraints (40.9%), adverse effects (19.7%), satisfaction with vision (6.6%) and negative advice (2.2%) from family and friends as reasons for not opting for keratorefractive surgery. These were also similar to the findings in the literature [1,5,10-12]. This may be due to the low level of awareness earlier discussed in this study. Lack of awareness may lead to a lack of information about keratorefractive surgery, thereby increasing the fear of having the surgery. The limited records of success rates and the perceived poor health system in Nigeria may increase mistrust among individuals, increasing fear and making them not willing to accept the procedure. The surgery may not be readily affordable for everyone due to the high cost of having the surgery done. Some participants in this study on focused group discussions and in-depth interviews, viewed it as surgery for the financially privileged, which may decrease the tendency of having the surgery done. There is a possibility of still using spectacles even after the surgery, especially the very high myopes. This may affect the uptake of the surgery, such that some individuals may view it as needless, which was seen from the findings in this study. Some individuals may be satisfied with their vision especially the low myopes, thereby seeing no need for keratorefractive surgery.
Conclusion
The willingness to accept keratorefractive surgical services in this study was low. The significant predictor of willingness to accept keratorefractive surgery was high myopia. The main barriers to the uptake of the services were fear of damage, lack of awareness and financial constraints while the reasons for uptake were tired of using spectacles, not wanting to use spectacles, beautification and career reasons. There is a need for patient education to improve surgical uptake.
Acknowledgments
I want to express my gratitude to my research team, Dr. Emenike, Dr. Kelechi, and Dr. Nduka, for their dedication and hard work during the field work. I would also like to extend a special thanks to my colleagues and friends for their encouragement and support throughout this endeavor.
Additionally, I am grateful to the management and staff of Eye Foundation Hospital Group for granting me permission and providing the necessary platform to conduct this study.
Lastly, I appreciate all the participants who volunteered to take part in this study.
Declaration
- Ethics approval and consent to participate
This study was carried out following the guidelines as contained in the declaration of Helsinki and approval was obtained from the Ethics and Research Committee of the Lagos State University Teaching Hospital, Ikeja, Lagos, Nigeria
- Consent for publication
Written informed consent for publication of participants clinical details were obtained.
- Competing interests
The authors have no relevant financial or non-financial interests to disclose
- Funding
The authors declare that no funds, grants, or other support were received during the preparation of this manuscript
References
- Ang RET, Camus EE, Rivera MCR, Vizconde DC, Canilao LMB, et al. (2015) Demographic and Clinical Profile of Patients who Underwent Refractive Surgery Screening. Philip J Ophthalmol 40: 64-71.
- Abraham EG, Megbelayin EO (2015) Pattern of Refractive Errors Among Ophthalmic Outpatients of University of Uyo Teaching Hospital, Uyo, Nigeria. Nigerian Journal of Ophthalmology 23: 39-43.
- Ajayi IA, Omotoye OJ, Omotoso-Olagoke O (2018) Profile of refractive error in Ekiti, south western Nigeria. Afr Vision Eye Health 77: 415.
- Holden BA, Fricke TR, Wilson DA, Jong M, Naidoo KS, et al. (2016) Global Prevalence of Myopia and High Myopia and Temporal Trends from 2000 through 2050. Ophthalmology 123: 1036-1042.
- Xu K, McKee HD, Jhanji V (2013) Changing perspective of reasons for not performing laser-assisted in situ keratomileusis among candidates in a university eye clinic. Clin Exp Optom 96: 20-24.
- Bamashmus MA, Saleh MF, Awadalla MA (2010) Reasons for not performing keratorefractive surgery in patients seeking refractive surgery in a hospital-based cohort in “Yemen.” Middle East Afr J Ophthalmol 17: 349-353.
- Gupta N, Naroo SA (2006) Factors influencing patient’s choice of refractive surgery or contact lenses and choice of centre. Cont Lens Anterior Eye 29: 17-23.
- McGhee CNJ, Craig JP, Sachdev N, Weed KH, Brown AD (2000) Functional, psychological, and satisfaction outcomes of laser in situ keratomileusis for high myopia. J Cataract Refract Surg 26: 497-509.
- Khan-Lim D, Craig JP, McGhee CN (2002) Defining the content of patient questionnaires: reasons for seeking laser in situ keratomileusis for myopia. J Cataract Refract Surg 28: 788-794.
- Ayanniyi AA, Olatunji FO, Hassan RY, Adekoya BJ, Monsudi KF, et al. (2013) Awareness and attitude of spectacle wearers to alternatives to corrective eyeglasses. Asian J Ophthalmol 3: 86-94.
- Naroo SA, Shah S, Kapoor R (1999) Factors That Influence Patient Choice of Contact Lens or Photorefractive Keratectomy. J Refract Surg 15: 132-136.
- Torricelli AA, Bechara SJ, Wilson SE (2014) Screening of refractive surgery candidates for LASIK and PRK. Cornea 33: 1051-1055.
Citation: Chidubem AO, Ebiem OP (2023) Willingness to Accept Keratorefractive Surgery and its Barriers among Myopes at Eye Foundation Hospital Group, Nigeria. J Ophthalmic Clin Res 10: 113.
Copyright: © 2023 Agu Obiajulu Chidubem, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.