A Rare Case of Isolated Sigmoid Colon Perforation in Patient with Blunt Trauma Abdomen
*Corresponding Author(s):
Ahmed Siddique AmmarSenior Registrar General Surgery, Mayo Hospital Lahore, Pakistan
Tel:03339981912,
Email:asammar1912@gmail.com
Abstract
A 47 years old male presented to emergency department with history of pain abdomen after road traffic accident 6 hours back. He had deceleration injury while driving a minivan when he hit a truck parked on road side. On presentation, his Airway and breathing was intact with GCS 15/15.Pulse was 110/min and blood pressure was 100/70 mmHg. His abdomen was generalized tender, mostly in the hypogastrium. Digital rectal examination was normal. Ultrasound abdomen showed free fluid in the peritoneal cavity and chest and abdominal X-rays were unremarkable. On opening the abdomen there was 7×7 cm isolated perforation in sigmoid colon 5 cm proximal to recto sigmoid junction. Repair of perforation was done and proximal double barrel sigmoid colostomy was made. Patient was discharged on 3rd post-operative day. Later after 4 months reversal of sigmoid colostomy was done and patient was discharged.
Keywords
Blunt Trauma Case Report; Colon; Colostomy; Deceleration; Sigmoid
ABBREVIATIONS
GCS: Glasgow coma scale
BACKGROUND
Isolated colon injuries are reported very rarely in literature. In blunt trauma abdomen the most commonly injured organs are solid viscera’s like liver and spleen followed by those parts of gut which are fixed e.g. duodenum [1]. Small gut injuries also get damaged in blunt trauma abdomen along with tear of mesentery of small intestine in deceleration injuries. However due to safe location and fixity of sigmoid colon in pelvis, isolated sigmoid colon injury is least likely. Moreover, due to fixity of sigmoid colon on the posterior wall, any blunt abdominal trauma that occurs will ultimately damages the small intestines first [2]. The low incidence of sigmoid colon injury due to blunt abdominal trauma and the lack of a definitive diagnostic method can lead to delay in diagnosis and treatment, subsequently resulting in high morbidity and mortality [3].
We presented a case where patient having road traffic accident had only isolated perforation of sigmoid colon while rest of every solid and hollow organs were normal.
CASE PRESENTATION
A 47-year-old male, driver by profession, presented in emergency department of EAST Surgical ward, MAYO Hospital Lahore with complaint of abdominal pain after road traffic accident 6 hours back. He had deacceleration injury while driving a minivan when he hit a truck parked on the road side. On presentation in emergency department, his airway and breathing were normal with Glasgow Coma Scale of 15/15. His pulse was 110/min and blood pressure were 100/70 mmHg. He was resuscitated, Nasogastric tube and Foley catheter passed. Digital rectal examination was normal with finger stained with stools. There was generalized tenderness in the abdomen with guarding in the lower abdomen. Bowel sounds were positive. Complete blood count was sent, total leucocyte count of 18×103 and hematocrit of 28%. Ultrasound abdomen showed to have minimal free fluid in the pelvis. Chest x-ray and abdominal x-ray were unremarkable. Plan of exploratory laparotomy was made with suspicion of peritonitis due to small gut perforation or mesenteric tear. After taking informed and written consent and arrangement of 2 pints of blood patient was explored under general anesthesia. On opening the abdomen through midline umbilical saving incision, there was gush of air along with approximately 500 ml of feculent fluid from the pelvis. Stomach duodenum and all the solid viscera were normal. There was 7×7 cm isolated perforation of sigmoid colon 5 cm proximal to recto sigmoid junction (Figure 1&2). The margins of the perforation were gangrenous. Abdomen washed with 5 liters of normal saline, margins of perforation freshened and perforation was closed with prolene 3/0 in single layer extra mucosal fashion. Descending colon was exteriorized as double barrel colostomy as diversion. Drain placed in pelvis and abdomen closed with prolene 1 continuous technique. Surgery and post-operative recovery were uneventful and patient was discharged on 3rd post-operative day. After 4 months distal logogram was done which showed normal distal colon and rectum. Reversal of double barrel colostomy wad done in elective operation theater and patient was discharged on 4th post-operative day.
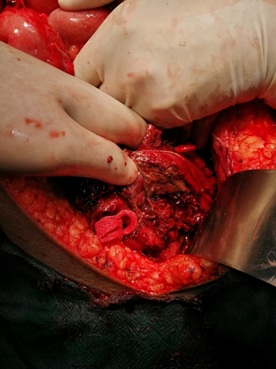 Figure 1: Perforation of sigmoid colon.
Figure 1: Perforation of sigmoid colon.
 Figure 2: Perforation of sigmoid colon. Margins of perforation are irregular.
Figure 2: Perforation of sigmoid colon. Margins of perforation are irregular.
DISCUSSION
The occurrence of colonic injuries caused by the blunt trauma are reported to be less than 1.1% in literature available. The most common cause of these colonic injuries is due to motor vehicle accidents while injuries due to direct blow or occupational trauma and falls are also reported [4].
In a study done by Öztürk et al. on 64 patients with colonic injury showed that 32 patients (50%) of colonic injuries are due to motor vehicles while 13 patients (20.3%) had history of fall from height and 7 patients (10.9%) had history of assault [5]. Colonic injuries are most commonly occurred after penetrating abdominal trauma while their incidence is very low in blunt abdominal trauma. Barden et al presented a case of isolated colon perforation due to bull hitting a patient from front. Another case reported by Ciftci et al. of colonic perforation due to intra vehicular accident [6].
Few studies showed isolated transverse colon perforation due to blunt trauma abdomen while only a few studies have been found in literature to report isolated sigmoid colon perforation due to blunt trauma abdomen. A large number of colonic injuries which are caused by blunt trauma abdomen can be very destructive and often associated with multiple organ damage with deteriorated clinical conditions [6]. The diagnosis of gastrointestinal injury due to blunt trauma face many clinical delays and is often very difficult and unreliable due to presence of other injuries and injuries to head and spinal cord, shock particularly in children [7].
In a patient in which a colonic injury in suspected the most important thing that affects the outcome is the time interval between admission in the emergency department and surgery. Shorter the duration less will be the morbidity and mortality in the post-operative period [8].
Clinically, abdominal tenderness, guarding, distension and abdominal wall contusion are important findings to suspect the intestinal injury. Plain abdominal X-rays, though performed routinely don’t give much information even in severe injury. Abdominal ultrasound can tell free fluid in the abdomen and interloop fluid and in the absence of any other solid organ injury it shows the injury to the gut. Complication rate of colonic injuries are very hazardous and may cause increased mortality if the duration is longer than 24 hours after injury. Still no single method is available which can accurately diagnose the isolated colon injury caused by blunt trauma abdomen though CT abdomen and pelvis give a good idea regarding the injury. Many studies emphasize the importance of repeated physical examinations of abdomen and observation in diagnosing the colonic injury in first 6 hours during which the signs of peritonitis appear. Digital rectal examination also plays an important role in diagnosis as finger stained with blood along with abdominal tenderness give a strong clue to colonic injury. The proposed reasons which cause the isolated sigmoid perforation in blunt trauma abdomen are the redundant sigmoid colon with long and wide mesentery and loaded colon which on sudden impact get perforated.
Many treatment options are available depending upon the severity of peritonitis. Primary repair is suitable for the injuries involving less than 50% of the colonic wall and with stable vital signs of patient while resection and anastomosis is suitable for the patients when the tissue loss is more than 50% and when there is extensive mesenteric injury causing decreased blood supply to colon and with unstable vital signs. The length of segment involved and grade of peritonitis also plays an important role with end colostomy is also an option when distal stump of colon can be exteriorized.
CONCLUSION
Isolated sigmoid colon perforation after blunt trauma is found very rare in literature and very few case reports are reported. This case report helps in better understanding of sigmoid colon injuries after blunt trauma abdomen.
SUMMARY OF THE CASE
|
1 |
Patient (gender, age) |
47-year male |
|
2 |
Final Diagnosis |
Isolated sigmoid colon perforation |
|
3 |
Symptoms |
Generalized tenderness in abdomen with guarding, absent bowel sounds. |
|
4 |
Medications |
Intravenous antibiotics, fluids. |
|
5 |
Clinical Procedure |
Exploratory laparotomy and double barrel colostomy |
|
6 |
Specialty |
General surgery |
CONSENT OF PATIENT
Written consent was obtained from the patient.
CONSENT OF ETHICS
Ethical approval is not required at out institution to publish case report.
CONFLICT OF INTEREST
The authors declare that there is no conflict of interest regarding the publication of this Case Report.
REFERENCES
- Chaubey D, Verma AK, Pandey A, Gupta A (2017) Isolated rectal perforation presenting as peritonitis in a child with enteric fever. JCS 7: e120-e122.
- Ho T, Chang SW, Yeh HW, Yeh CB (2017) Occult perforation with circumferential ischaemic injury of the sigmoid colon following seat-belt trauma: a case report. HKJ 24: 100-103.
- Pinto A, Scaglione M, Giovine S, Romano S, Lassandro F, et al. (2004) Comparison between the site of multislice CT signs of gastrointestinal perforation and the site of perforation detected at surgery in forty perforated patients. Radiol Med 108: 208-217.
- Singh M, Dalal S, Amandeep VS (2017) Delayed Presentation of an Isolated Sigmoid Colon Injury Fol-lowing Blunt Abdominal Trauma: A Case Report & Review of Literature. J Med Case Rep 6:247.
- Ozturk MA, Erdik B, Eren OO (2016) Sigmoid Colon Perforation Related to Bevacizumab in a Patient With Glioblastoma. Am J Ther 23: e241-e242.
- Ciftci F, Benek S, Kezer C (2016) A Rare Cause of Mechanical Intestinal Obstruction: A Neoplastic Intra-Abdominal Testis. Int Surg 101: 167-170.
- Tiwari A, Sharma H, Qamar K, Sodeman T, Nawras A (2017) Recognition of extraperitoneal colonic perforation following colonoscopy: a review of the literature. Case Rep Gastroenterol 11: 256-264.
- Wakodkar AA, Singh AD, Mesharm HM (2019) Descriptive study of isolated bowel injury following blunt trauma abdomen. Indian J Appl Res 9: 12-13.
Citation: Ammar AS, Khalid R, Saeed S, Naqi SA (2020) A Rare Case of Isolated Sigmoid Colon Perforation in Patient with Blunt Trauma Abdomen. J Emerg Med Trauma Surg Care 7: 053
Copyright: © 2020 Ahmed Siddique Ammar, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.