Anesthetic Tracheal Wound Per-Intubation before Total Thyroidectomy and Lymphadenectomy Surgical Procedure: A Case-Report and Review
*Corresponding Author(s):
Rougier GHead And Neck Oncologic Surgery Department, Curie Institute, PSL Research University, Paris, France
Tel:+33 0619948047,
Email:guillaumerougier75@gmail.com
Abstract
Background: Tracheal tears along thyroidectomy are rare but severe complications.
Case presentation: A 59 years-old patient was diagnosed during anterior lymphadenectomy procedure with total thyroidectomy with a tracheal posterior wound, between 1st and 2nd cartilage ring, caused by the specific mandrel-tube used for recurrent laryngeal nerve monitoring during intubation. Patient then presented with bilateral pneumothorax, pneumomediastinum, and septic syndrome caused by cervical infected hematoma expanding to the chest, managed with draining chest tubes and systemic antibiotics. Finally, the patient discharged home on POD twelve.
Conclusion: It seems important that practitioners, anesthetists and surgeons be aware of such a complication, as it can engage the patient short-term life prognosis and risk of tracheal sequelae, as well as recurrent nerve laryngeal palsies.
Keywords
Intubation complication; Monitoring tube; NIM; Thyroidectomy; Tracheal wound
INTRODUCTION
Intubation related tracheal wounds and ruptures are rare, but still life-threatening complication [1,2]. Depending on their size and location, they can be managed surgically with immediate repair or conservatively with acute surveillance [3]. Many causes have been described, but to our knowledge, few tracheal wounds are specifically caused by the mandrel used for intubation. We report here the case of a mandrel-related tracheal wound, assessed during neck surgery.
DESCRIPTION OF THE CASE
We report here the case of 59 years-old woman whom has undergone total thyroidectomy with anterior, left carotid and jugular lymph node excision for a left papillary thyroid carcinoma with multiples left sided lymphadenopathies. She hadn’t any relevant past medical or surgical history and presented with healthy overall health.
Surgical procedure and tracheal tear assessment
Surgical procedure consisted in a classic total thyroidectomy with neck dissection for excision of anterior, left jugular and carotid lymph nodes with preservation of laryngeal recurrent nerves. Nerve Intraoperative Monitoring (NIM-Response@ Medtronic-Minneapolis, Minnesota, USA) device was used with the specific intubation tube. A posterior tracheal wound was assessed during anterior lymphadenectomy procedure, seeing the tracheal tube cuff behind cartilage rings with clear posterior rupture of the tracheal membrane (Figure 1).
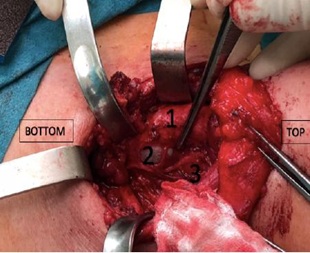 Figure 1: Assessed tracheal wound during surgery, with balloon-tube exposure.
Figure 1: Assessed tracheal wound during surgery, with balloon-tube exposure.
1.Anterior tracheal wall 2. Balloon tube exposure 3. Laryngeal recurrent nerve
It was immediately decided not to perform any surgical repair or suture, therefore ending the procedure with left jugular and carotid lymphadenectomy. Cervical suction drainage was initiated with two cervical drains.The assessed wound was totally posterior, at the junction between cartilage and tracheal membrane, 1.5 cm large, between 1st and 2nd cartilage ring, below thyroid cartilage. Pressure inside the cuff was checked out and no hyper pressure was assessed. After immediate concentration with our senior anesthetist, it is most certain that this wound happened during intubation with the specific mandrel used for recurrent laryngeal nerve monitoring tube.
Post-operative management
During immediate post-operative period, sub-cutaneous cervical emphysema with dyspnea and respiratory failure have been observed, due to bilateral pneumothorax and pneumomediastinum diagnosed after chest standard X-ray and CT-scanner (Figures 2 and 3).
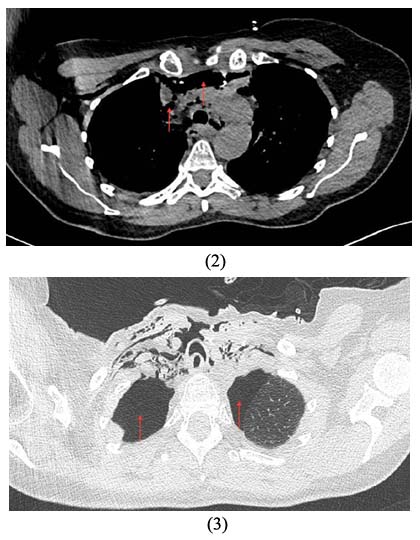 Figures 2 and 3: Tracheal wound with bilateral pneumothorax, pneumomediastinum and esophagus hernia.
Figures 2 and 3: Tracheal wound with bilateral pneumothorax, pneumomediastinum and esophagus hernia.
Cervical suction drainage was eventually a failure and immediate chest tube drainage has been performed in the post-anesthesia care unit with favorable outcome. Then, the patient discharged to ICU for post-operative surveillance. Trans-nasal endoscopy showed an important anterior hernia of the esophagus through the wound that was measured to 5 cm length, thus explaining coughing, inhaling and swallowing troubles with slight liquid-related dysphagia.
At POD 5 CT-scanner showed total regression of the right pneumothorax, slight persistent left pneumothorax, and major hematoma expanding throughout the neck to the mediastinum. Removal of all the drains were performed at POD 6 and patient discharged to conventional hospitalization unit. Septic signs with inflammatory biologic syndrome led to another imaging control with CT-scanner that showed the appearance of an air-fluid level at the upper part of the hematoma located right next to the lymphadenectomy surgical site with retro-sternal infiltration (Figure 4).
 Figure 4: Infected neck and mediastinum hematoma.
Figure 4: Infected neck and mediastinum hematoma.
Decision was made not to perform a surgical drainage given the overall well tolerance, and to initiate systemic broad-spectrum antibiotics. All bacteriologic samples including surgical site puncture and blood cultures were negative, and the patient finally discharged home after regression of both fever and inflammatory biologic syndrome at POD 12.
No other surgery side effects or anesthetic complications were noticed, and clinical signs including swallowing troubles and dysphagia had disappeared. Six months later, a left laryngeal immobility was still observed without further abnormalities.
DISCUSSION
Tracheal wall disruption, wounds or lacerations are rare and severe complications. Traumatic intubation is the first iatrogenic etiology [1]. Although it seems to be a known condition along thoracic surgical procedures [2,3], assessing the tracheal tear during the surgical procedure by seeing the protrusion of the cuff tube within the surgical field is exceptionally rare along cervical surgeries. Nevertheless, there are a relevant number of articles referring to tracheal wounds and lacerations during neck surgeries in the literature.
Similar cases in the literature
Thiam & Al. report three patients similar to our own, with per-operative assessment of the cuff tube in the cervical surgical field [4]. The tracheal tear was also posterior and lateral, without complete rupture. Two patients have undergone immediate surgical repair with direct suture, and one had a conservative management with suction drainage, without any other complications, as our patient.
Many articles in the literature report various risk factors regarding tracheal tears, divided in two kinds, anatomical (that include congenital or acquired tracheal abnormalities, chronic steroid use, female sex, advanced age, tracheal and bronchial chronic diseases, smoking abuse) or mechanical (over sizing of the tube, over distention of the cuff tube, emergency cases…) [1]. However, it seems important to our team to specify that along such risk factors, the use of an introducer significantly increases the chances for a tracheal rupture, as it can directly injure and penetrate the inner mucosa and muscular posterior layer. In our reported case, the risk factor could be the gender, anatomical specificities like a long and thin neck and the use of an intubation introducer.
Sahin & Al. report two cases of tracheal posterior and lateral lacerations during intubation caused specifically by an introducer and assessed during the procedure, successfully treated with a conservative treatment [5]. Also, the use of an introducer is often necessary because of difficult intubation criteria, (limited mouth opening, radiotherapy history, large and short neck), thus hardening the procedure and increasing chances for a tracheal rupture. Last but not least, due to the flexibility of the neuro-monitoring tracheal tube, introducers often happen to be unavoidable in such procedures.
In a logical way, the posterior and lateral membranous part of the tracheal wall is the first concerned by such wounds [3,4,6-8], as the anterior part essentially made of cartilage is more resistant and solid. However, Warner & Al. report in their article an anterior tracheal laceration after a routine endotracheal intubation, likely caused by an introducer which was located beyond the distal orifice of the tube [1].
Xu & Al. also report the case of 51 years-old woman whom has undergone total thyroidectomy under laryngeal recurrent nerves monitoring, with an anterior tracheal rupture diagnosed during surgery [9]. Such cases enlighten the fact that as introducers can be held responsible for any kind of tracheal tears, anywhere, and they have to be very carefully manipulated.
If it seems true that so-called tracheal wounds caused by over distension or over sizing of the tube can be in fact assimilated to a tracheal wall disruption without systematic air-leak linked symptoms, introducer-related true ruptures often lead to major cervical and thoracic signs and life-threatening complications, as for our patient.
Airway and tear management
Immediate surgical repair has often been considered the best option [2,7,9], based on the hypothesis that it might allow a safe extubation along with a shortened healing time. Direct suture or myovascular transposition flap seem to be the most performed surgical procedures, in that case [7].
Of course, as we can only evaluate such complications throughout retrospective studies, it remains unclear which treatment offers the best healing chances, and to define a gold standard. Xu & Al report in their article an immediate surgical repair by right thoracotomy, along with a thoracic surgical team, as the tear was anterior, 7 cm long, and remained unreachable with a classic retro-sternal approach [9]. In their review of the literature, which included 208 patients, all patients diagnosed with tracheal rupture during surgery underwent immediate surgical repair, whereas others underwent conservative management if the tear was 2 cm or less along with a stable clinical situation.
This remains close to the global management described in the literature over such important tracheal tears [1-3] but in our case, with a postero-lateral and small disruption, without true rupture assessed, conservative management seemed to be the best option, even if diagnosed during surgery, and regardless of post-operative inherent complications. Such a conservative treatment includes early extubation, cervical suction drainage that must be continued as long as possible, low-pressure ventilation if any is required, vocal-fold rest and enteral nutrition. Re-intubation must be avoided at any cost, as it often results in worsened wounds in an emergency context, with a hardened surgical procedure.
In that case, tracheostomy should be performed by the senior surgeon that first assessed the tear, in order to avoid a complete tracheal section. Stenting procedures have been performed in such cases, as report Marchese & Al. after a double-lumen intubation procedure, with a successful course [2]. Nevertheless, with a reported overall mortality of 19.2%, tracheal rupture is a life-threatening complication and precise criteria should be proposed to evaluate the need for surgical repair or conservative management [8-10].
DECLARATIONS
Ethics approval and consent to participate: The patient has given full written consent to participate and to publish this study, surgical pictures and radiologic examinations figures included.
Consent for publication: The patient has given full written consent to publish this study, surgical pictures and radiologic examinations figures included.
Availability of data and materials: All data generated during this study are included in this published article.
Competing interests: The authors declare that they have no competing interests.
Author’s contribution: Rougier G: Main author, Lesnik M: This author helped in a minor contribution, Badois N: This author helped in a minor contribution, Canu G: This author helped in a minor contribution, Aseguin-Givelet: This author helped in a minor contribution, Dhonneur G: This author helped in a minor contribution, Choussy O: This author helped in a major contribution. All authors have read and approved the final version of this manuscript.
REFERENCES
- Warner MA, Fox JF (2016) Direct Laryngoscopy and Endotracheal Intubation Complicated by Anterior Tracheal Laceration Secondary to Protrusion of Preloaded Endotracheal Tube Stylet. A A Case Rep 6: 77-79.
- Marchese R, Mercadante S, Paglino G, Agozzino C, Villari P, et al. (2012) Tracheal stent to repair tracheal laceration after a double-lumen intubation. Ann Thorac Surg 94: 1001-1003.
- Óvári A, Just T, Dommerich S, Hingst V, Böttcher A, et al. (2014) Conservative management of post-intubation tracheal tears-report of three cases. J Thorac Dis 6: 85-91.
- Thiam NF, Diom ES, Ndiaye C, Sy A (2017)Plaies Trachéales Post Intubations Dans La Chirurgie Cervicale: À Propos de 3 Cas. Pan Afr Med J 28: 168.
- Sahin M, Anglade D, Buchberger M, Jankowski A, Albaladejo P, et al. (2012) Case reports: iatrogenic bronchial rupture following the use of endotracheal tube introducers. Can J Anaesth 59: 963-967.
- Ceylan KC, Kaya SO, Samancilar O, Usluer O, Gursoy S, et al. (2013) Intraoperative management of tracheobronchial rupture after double-lumen tube intubation. Surg Today 43: 757-762.
- Escott AB, Pochin RS (2016) Repair of a Posterior Perforation of the Trachea Following Thyroidectomy with a Muscle Transposition Flap. Ear Nose Throat J 95: 14-17.
- Tartaglia N, Iadarola R, Lascia AD, Cianci P, Fersini A, et al. (2018) What is the treatment of tracheal lesions associated with traditional thyroidectomy? Case report and systematic review. World J Emerg Surg 13:15.
- Xu X, Xing N, Chang Y, Du Y, Li Z, et al. (2016) Tracheal rupture related to endotracheal intubation after thyroid surgery: a case report and systematic review. Int Wound J 13: 268-271.
- Sanna S, Monteverde M, Taurchini M, Mengozzi M, Genestreti G, et al. (2014) It could suddenly happen: delayed rupture of the trachea after total thyroidectomy. A case report. G Chir 35: 65-68.
Citation: Rougier G, Lesnikm M, Badois N, Canu G, Aseguin-Givelet, et al. (2019) Anesthetic Tracheal Wound Per-Intubation before Total Thyroidectomy and Lymphadenectomy Surgical Procedure: A Case-Report and Review. J Anesth Clin Care 6: 41.
Copyright: © 2019 Rougier G, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.