Case Report: Ultrasound Assisted Removal of Broken Intra-Arterial Catheter
*Corresponding Author(s):
Chih-Cheng WuDepartment Of Anesthesiology, Taichung Veterans General Hospital, Taichung, ROC, Taiwan
Tel:+886 423592525,
Fax:+886 423595046
Email:chihcheng.wu@gmail.com
Abstract
Damage to an intra-arterial catheter is a rare complication following successful catheterization. The removal of a broken intra-arterial catheter was difficult and required assistance of facilities outside the operation room before. We used the ultrasound to localize a disrupted intra-arterial catheter and continuously traced the flowed catheter with changing location in the radial artery. After serial explorations the surgeon successfully removed the disrupted catheter from the deep palmar artery arch. We also reviewed previously reported cases and summarized the roles of ultrasound in assisting the procedures.
Keywords
Arterial Catheter, radial artery, palmar artery
INTRODUCTION
The technique of peripheral arterial catheterization used for hemodynamic monitoring is commonly applied in clinical practices. The catheter is often cannulated into the radial artery, and complications may occur during the catheterization [1,2]. Reported complications were temporary occlusion of the radial artery, and the formation of hematoma or bleeding at the puncture sites. Less commonly found complications include the formation of pseudoaneurysm, abscess, cellulitis, injury of the median nerve, suppurative thrombarteritis, air embolism, compartment syndrome and carpal tunnel syndrome [1]. Here, we reported a rare case with damage to the catheter in the radial artery during removal.
CASE REPORT
This 87-year-old male patient was diagnosed sigmoid colon cancer and hwas admitted to receive anterior resection. Because of his old age and past history of uncontrolled hypertension, a 22-gauge cannula (BD Insyte, Singapore) was inserted in the left radial artery for continuous monitoring the blood pressure perioperatively. After uneventful insertion, this catheter was secured to the skin with a Tegarderm transparent dressing (3M Health Care, St. Paul, MN, USA). The surgery was performed uneventfully and the endotracheal tube was also weaned at the end of the surgery.
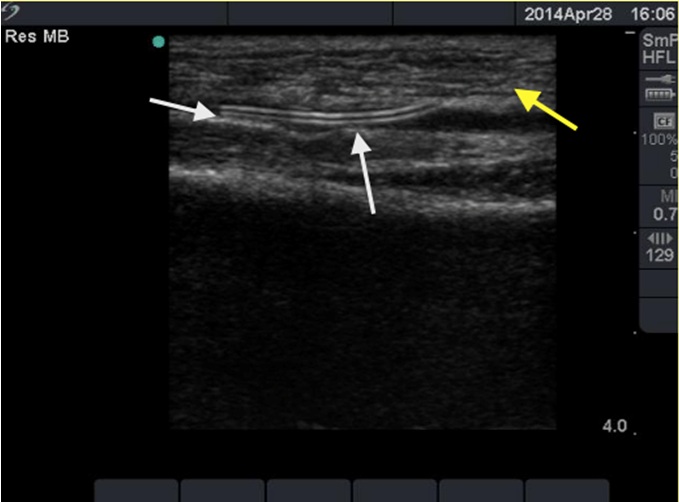
However, during removal of the intra-arterial catheter in the Post-Anesthesia Room (PAR), the catheter was found to break with a residual in the radial artery. To investigate the broken catheter, we used an ultrasound system (SonoSite MicroMaxxTM) with a linear 38 mm, 6-13 MHz transducer via the longitudinal view. The echogenicity produced by the retained part could be visualized just below the skin near the insertion site and the whole length could also be visualized (Figure 1 with arrows). When we localized the broken catheter, emergent surgery to remove the broken catheter was immediately scheduled by the cardiovascular surgeons. After exploring the skin around the insertion site and the predicted location of the residual catheter by the ultrasound, the radial artery was explored but the retained broken catheter was absent. Further ultrasound examination was performed and the broken catheter was noted to be flowed distally, and further exploration at the distal forearm near the wrist was performed. Unfortunately, the catheter was still absent. The ultrasound was used again and the broken catheter was located more distally in the deep palmar artery arch. After further deep exploration, the broken catheter (Figure 2) was successfully removed through the final incised wound without complications.

DISCUSSION
Radial artery cannulation for arterial pressure monitoring is a valuable adjunct for patients receiving anesthesia for complicated and major surgeries and receiving respiratory support in the intensive care unit [2,3]. Damage to this intra-arterial catheter is a rare complication following catheterization [4]. Disruption of the catheter during removal with a residual part retained in the radial artery following a successful placement has been rarely reported [5-9].
It is well known that the intra-arterial fragment may be flowed away by the blood flow and it could be considered that we should explore distally to find the intra-arterial fragment [5]. We needed tools to make sure the correct incision site where we should explore. Several tools has been reported to localize the broken catheter include 3-dimensional Computerized Tomography (CT) [6], ultrasound [7,8] and plain radiography [9]. However, assistance using radiological modalities such as CT and plain radiography is not immediately accessible and cannot be applied intraoperatively and continuously during surgeries in most operation rooms. Even if a residual part of the intra-arterial catheter can be successfully localized by CT or plain radiography outside the operation room, it may be flowed elsewhere when the patients were transported to the operation room to receive surgical explorations. Furthermore, plain radiography only provides a low resolution and is therefore not an optimal modality for localizing the broken catheters [9]. In our patient, due to the arterial blood flow, the broken catheter was apparently moved several times during the exploration procedure before it was finally removed in the deep palmar region. In this case by aid of ultrasound we could quickly and continuously trace the changing positions of the broken catheter, and the surgeon could successfully remove the retained part.
Moody [7] has proposed that ultrasound offers a number of advantages for localizing a broken catheter, as it can provide information about the exact location of the cannula fragment, which minimizes the exploration time and surgical field, and it allows the ability to monitor the fragment in real time.
In this case we proposed another advantage of ultrasound to survey the intravascular foreign body in its continuous monitoring with changing locations. The intra-arterial catheter fragment was continuously transported by blood flow into the distal and deep palmar regions, and was absent in serial explorations in the skin and vessel. Without ultrasound to continuously trace the broken catheter along the artery and its distribution, we could not confirm that distal migration and could not assist the surgeon to find it.
In summary, ultrasound is a valuable and convenient tool to localize the broken catheter fragment that may migrates by the arterial blood flow and is difficult to be localized.
REFERENCES
- Bengezi OA, Dalcin A, Al-Thani H, Bain JR (2003) Unusual complication of radial artery cannulation. Can J Plast Surg 11: 213-215.
- Scheer BV, Perel A, Pfeiffer UJ (2002) Clinical review: complications and risk factors of peripheral arterial catheters used for haemodynamic monitoring in anaesthesia and intensive care medicine. Crit Care 6: 199-204.
- Hutton P, Prys-Roberts C (1994) Monitoring in Anaesthesia and Intensive Care. WB Saunders, London, England. Pg no: 134-138.
- Ho KS, Chia KH, Teh LY (2003) An unusual complication of radial artery cannulation and its management: a case report. J Oral Maxillofac Surg 61: 955-957.
- Shah US, Downing R, Davis I (1996) An iatrogenic arterial foreign body. Br J Anaesth 77: 430-431.
- Luo CF, Mao CC, Su BC, Yu HP (2010) An iatrogenic complication of radial artery cannulation. Acta Anaesthesiol Taiwan 48: 145-147.
- Moody C, Bhimarasetty C, Deshmukh S (2009) Ultrasound guided location and removal of retained arterial cannula fragment. Anaesthesia 64: 338-339.
- Ball DR, Stott SA, Rouse R (1996) Locating an arterial foreign body by ultrasonography. Br J Anaesth 77: 811.
- Brown MM (1991) Another complication of arterial cannulation. Anaesthesia 46: 326.
Citation: Kuan-Hung C, Wu C-C, Chi-Jen H (2016) Case Report: Ultrasound Assisted Removal of Broken Intra-Arterial Catheter. J Anesth Clin Care 3: 016.
Copyright: © 2016 Chih-Cheng Wu, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.