Clinical Image-Superior Mesenteric Vein Syndrome
*Corresponding Author(s):
Lauren RaffDepartment Of General Surgery, Health Care Hernia Center, The University Of North Carolina, Chapel Hill, NC, United States
Tel:919-966-4389,
Fax:919-966-0389
Email:lauren_raff@med.unc.edu
Clinical Image
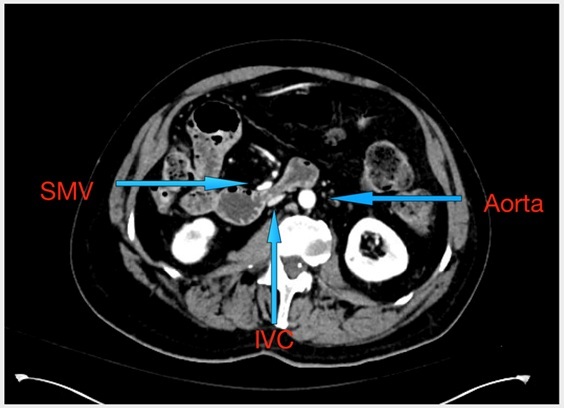
A 59 year old male with history of cerebral palsy presented with a 5-day history of abdominal pain, distension, nausea, and vomiting. He underwent a CT scan without a distinct transition point causing bowel obstruction. The patient was admitted and underwent an esophagogastroduodenoscopy (EGD), which confirmed extrinsic compression of the duodenum. Upon further review of the CT scan, it was noted that there was mild compression at the third and fourth portions of the duodenum between vascular structures, and not the expected structures of the aorta and superior mesenteric artery. The patient was taken to the operating room and underwent diagnostic laparoscopy with laparoscopic mobilization of the right colon and the entire duodenum to the ligament of treitz. Intra-operatively, the patient was found to have extrinsic compression of the duodenum between the inferior vena cava (IVC) and the superior mesenteric vein (SMV). The SMV was dissected off the anterior duodenum, creating space between these two structures and relieving the extrinsic compression. EGD was performed at the end of the case and the duodenum was successfully traversed endoscopically.
Citation: Raff L and Perez AJ (2020) Clinical Image-Superior Mesenteric Vein Syndrome. J Emerg Med Trauma Surg Care 7: 042
Copyright: © 2020 Lauren Raff, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.