Journal of Anesthesia & Clinical Care Category: Clinical
Type: Case Report
Continuous Erector Spinae Plane Block for Mammary Reconstruction after Mastectomy: Case Report
*Corresponding Author(s):
Maylane Oliveira MagalhãesAnesthesiologist Hgrs And Pain Physician At Santa Casa De Misericordia Da Bahia Salvador, Salvador, Bahia, Brazil
Email:dbomfim@gmail.com; maymagalhaes@icloud.com
Received Date: May 30, 2019
Accepted Date: Jun 03, 2019
Published Date: Jun 10, 2019
Abstract
Motivation and objectives
The diffusion of ultrasound machines with better resolutions and accessibility allowed its use in regional blocks, making the blocking of the interfascial planes a common procedure. Forero et al. 2016 describes for the first time the Erector Spinae Plane Block, this type of blockade has been shown effective in thoracic and abdominal surgeries. The objective of this report is to describe the use of a catheter for continuous perioperative anesthesia.
Case report
Patient with multiple drug allergies, with previous mastectomy, submitted to breast reconstruction, with continuous erector spinae plane block guided by ultrasound.
Conclusion
Effective postoperative continuous anesthesia, without the use of opioids.
The diffusion of ultrasound machines with better resolutions and accessibility allowed its use in regional blocks, making the blocking of the interfascial planes a common procedure. Forero et al. 2016 describes for the first time the Erector Spinae Plane Block, this type of blockade has been shown effective in thoracic and abdominal surgeries. The objective of this report is to describe the use of a catheter for continuous perioperative anesthesia.
Case report
Patient with multiple drug allergies, with previous mastectomy, submitted to breast reconstruction, with continuous erector spinae plane block guided by ultrasound.
Conclusion
Effective postoperative continuous anesthesia, without the use of opioids.
Keywords
Erector spinae plane block; ESP block; Mastectomy; Opioid free analgesia; Postoperative analgesia; Ultrasound guided block
INTRODUCTION
The development of several areas in medicine has been accompanied by the emergence of several anesthesia techniques, which promote greater safety, comfort and excellent postoperative recovery. The Erector Spinal Plane block (ESP) appears as one of these promising alternatives for postoperative pain relief. The first report and publication regarding this technique was made by Forero et al. in 2016 and its effectiveness was reported in four cases [1]. The local anesthetic is injected between the transverse process of the fifth thoracic vertebra (T5) and the erector muscle of the spine, with dispersion that can reach T1 to T9 levels. Few cases are reported with the placement of a catheter for postoperative analgesia. Firstly, it was reported for thoracic analgesia, but several authors have already used it for abdominal surgery [2,3]. The ESP block provides visceral analgesia in addition to somatic analgesia due to propagation into the paravertebral space [4].
CASE REPORT
A 34-year-old female patient, 51 kg, with diagnosis of breast neoplasm in 2016, submitted to radical mastectomy on the left, with previous lymphadenectomy, being proposed breast reconstruction with prosthesis implantation.
She reported allergy to dipyrone, acetyl salicylic acid, non-steroidal anti inflammatory, lactose, egg, red meat and swine. ASA I, without difficult airway predictors. Laboratory tests: Hemoglobin: 12.7, Hematocrit: 39%, PT: 95.9%, a TTP: 33.7 Platelets: 245 K, urea: 34.9, Creatinine: 0.65. ECG: altered ventricular repolarization.
Anesthesia was performed with Midazolam (5 mg), continuous infusion of Magnesium Sulfate (20 mg.kg-1.h-1) + Lidocaine without Vasoconstrictor (1 mg.kg-1.h-1) + Dexmedetomidine (1 mcg.kg-1.h-1) [“MLD”] at induction. Dexmedetomidine (0.5 mcg.kg-1.h-1) was maintained as the maintenance drug, all medications being administered intravenously.
Antibiotic prophylaxis with intravenous cefazolin 2g was also given. The intubation was preceded by intravenous induced, which was done with the maintenance of the continuous infusion of “MLD”, followed by additional administration of Propofol 120 mg + Lidocaine 50mg and Rocuronium 50 mg, all them intravenously.
After orotracheal intubation, the patient was positioned in right lateral decubitus, and then ESP block, at level of T5, was performed with a Tuohy needle 17 G for which was passed through an epidural catheter (PD) # 18 allowing the continuous local anesthetic’s infusion (Figure 1).
In our practice, usually the US guided peripheral nerve block is performed with a Mobinson M4 device, with the help of an iPad, which works like a screen. Following the US guided needle insertion, that was positioned in the ESP, a Ropivacaine 0, 75%, in a total amount of 20 ml, was administered through the needle, followed by the catheter insertion (Figures 2 and 3).
General Anesthesia was maintained by inhaled anesthetic administration, and Sevoflurane at 1 CAM was administered. In the postoperative period, a Levobupivacaine 0.25 % solution was given, in an infusion rate of 3 ml.h-1. In the immediate postoperative period, still in the CRPA, the patient was evaluated about recovery of Anesthesia, having reported no pain, which was assessed by VAS (Visual Analogue Scale - VAS) score, and then described as VAS 0.
The patient’s pain score was evaluated at 2h, 6h, 12h and 24h, that was reported like VAS 0, 1, 1 and 0, respectively. No opioids, in the postoperative period, were given.
She reported allergy to dipyrone, acetyl salicylic acid, non-steroidal anti inflammatory, lactose, egg, red meat and swine. ASA I, without difficult airway predictors. Laboratory tests: Hemoglobin: 12.7, Hematocrit: 39%, PT: 95.9%, a TTP: 33.7 Platelets: 245 K, urea: 34.9, Creatinine: 0.65. ECG: altered ventricular repolarization.
Anesthesia was performed with Midazolam (5 mg), continuous infusion of Magnesium Sulfate (20 mg.kg-1.h-1) + Lidocaine without Vasoconstrictor (1 mg.kg-1.h-1) + Dexmedetomidine (1 mcg.kg-1.h-1) [“MLD”] at induction. Dexmedetomidine (0.5 mcg.kg-1.h-1) was maintained as the maintenance drug, all medications being administered intravenously.
Antibiotic prophylaxis with intravenous cefazolin 2g was also given. The intubation was preceded by intravenous induced, which was done with the maintenance of the continuous infusion of “MLD”, followed by additional administration of Propofol 120 mg + Lidocaine 50mg and Rocuronium 50 mg, all them intravenously.
After orotracheal intubation, the patient was positioned in right lateral decubitus, and then ESP block, at level of T5, was performed with a Tuohy needle 17 G for which was passed through an epidural catheter (PD) # 18 allowing the continuous local anesthetic’s infusion (Figure 1).
In our practice, usually the US guided peripheral nerve block is performed with a Mobinson M4 device, with the help of an iPad, which works like a screen. Following the US guided needle insertion, that was positioned in the ESP, a Ropivacaine 0, 75%, in a total amount of 20 ml, was administered through the needle, followed by the catheter insertion (Figures 2 and 3).
General Anesthesia was maintained by inhaled anesthetic administration, and Sevoflurane at 1 CAM was administered. In the postoperative period, a Levobupivacaine 0.25 % solution was given, in an infusion rate of 3 ml.h-1. In the immediate postoperative period, still in the CRPA, the patient was evaluated about recovery of Anesthesia, having reported no pain, which was assessed by VAS (Visual Analogue Scale - VAS) score, and then described as VAS 0.
The patient’s pain score was evaluated at 2h, 6h, 12h and 24h, that was reported like VAS 0, 1, 1 and 0, respectively. No opioids, in the postoperative period, were given.

Figure 1: 1- local anesthetic over transverse process at erector spinae plane.
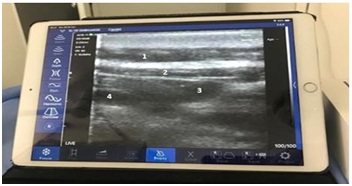
Figure 2: 1.Muscle trapezius / 2. Erector spine muscle / 3. e / 4. Transverse process.
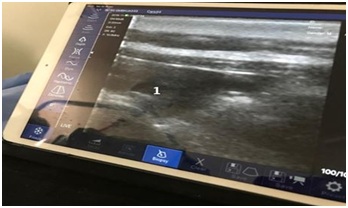
Figure 3: 1- Local anesthetic on erector spinae muscle.
DISCUSSION
Following the advances in ultrasound-guided approaches for regional analgesia, Interfacial plane blockades have become increasingly common. The most recent of these blockades already reported in the literature is the ESP blockade described by Forero et al. in 2016 [1].
The ESP block is indicated in pulmonary lobectomy, mastectomy, videothoracoscopy, axillary sentinel node biopsy, rib fractures and abdominal surgery [2,4]. In our case, the patient submitted to the blockade for breast reconstruction after mastectomy had multiple drug allergies, and opted for ESP blockade associated with anesthesia and opioid-free postoperative. Forero et al. reported a similar dermatomal level of sensory block [1,3].
One of the main advantages of peripheral blockades is avoiding the neuraxial approach, avoiding the numerous complications such as nerve damage, spinal hematomas or CNS infection, such as meningitis. The ESP block allows catheter insertion, which is important for continuous analgesia. In our case, effective postoperative analgesia was established by the catheter below the plane of the spinal erector muscle [5].
With this report, we conclude that ESP blockade is effective in promoting analgesia of several dermatomes at both the thoracic and abdominal levels. The sites of action of the ESP block are the dorsal and ventral branches of the thoracic spinal nerves and the paravertebral space. Based on Ueshima's work, 3 mL of local anesthetic is sufficient to cover a dermatome. In our report, we administered 20 ml of 0.75% ropivacaine intraoperatively, aiming to achieve analgesia from T1 to T9 dermatomal levels. However, other studies are necessary to understand if this proportion is adequate and to what extent the local anesthetic disperses during a continuous infusion [5].
The ESP block is reliable and simple to perform, it brings less neurological complications, mainly because of having minimal or even no contact with the neuroaxis. However, randomized clinical trials are needed to evaluate the efficacy of this blockade. The ESP block may be adequate for the treatment of acute and chronic pain, as it provides excellent analgesia via the catheter in the erector spinal plane.
The ESP block is indicated in pulmonary lobectomy, mastectomy, videothoracoscopy, axillary sentinel node biopsy, rib fractures and abdominal surgery [2,4]. In our case, the patient submitted to the blockade for breast reconstruction after mastectomy had multiple drug allergies, and opted for ESP blockade associated with anesthesia and opioid-free postoperative. Forero et al. reported a similar dermatomal level of sensory block [1,3].
One of the main advantages of peripheral blockades is avoiding the neuraxial approach, avoiding the numerous complications such as nerve damage, spinal hematomas or CNS infection, such as meningitis. The ESP block allows catheter insertion, which is important for continuous analgesia. In our case, effective postoperative analgesia was established by the catheter below the plane of the spinal erector muscle [5].
With this report, we conclude that ESP blockade is effective in promoting analgesia of several dermatomes at both the thoracic and abdominal levels. The sites of action of the ESP block are the dorsal and ventral branches of the thoracic spinal nerves and the paravertebral space. Based on Ueshima's work, 3 mL of local anesthetic is sufficient to cover a dermatome. In our report, we administered 20 ml of 0.75% ropivacaine intraoperatively, aiming to achieve analgesia from T1 to T9 dermatomal levels. However, other studies are necessary to understand if this proportion is adequate and to what extent the local anesthetic disperses during a continuous infusion [5].
The ESP block is reliable and simple to perform, it brings less neurological complications, mainly because of having minimal or even no contact with the neuroaxis. However, randomized clinical trials are needed to evaluate the efficacy of this blockade. The ESP block may be adequate for the treatment of acute and chronic pain, as it provides excellent analgesia via the catheter in the erector spinal plane.
REFERENCES
- Forero M, Adhikary SD, Lopez H, Tsui C, Chin KJ (2016) The Erector Spinae Plane Block: A Novel Analgesic Technique in Thoracic Neuropathic Pain. Reg Anesth Pain Med 41: 621-627.
- Chin KJ, Malhas L, Perlas A (2017) The Erector Spinae Plane Block Provides Visceral Abdominal Analgesia in Bariatric Surgery: A Report of 3 Cases. Reg Anesth Pain Med 42: 372-376.
- Forero M, Rajarathinam M, Adhikary S, Chin KJ (2017) Continuous Erector Spinae Plane Block for Rescue Analgesia in Thoracotomy After Epidural Failure: A Case Report. A A Case Rep 8: 254-256.
- Krediet AC, Moayeri N, van Geffen GJ, Bruhn J, Renes S, et al. (2015) Different Approaches to Ultrasound-guided Thoracic Paravertebral Block: An Illustrated Review. Anesthesiology 123: 459-474.
- Ueshima H, Hiroshi O (2018) Spread of local anesthetic solution in the erector spinae plane block. J Clin Anesth 45: 23.
Citation: de Azevedo VLF, Bomfim DVV, de Novaes TF, Filho EMC, Santana JC, et al. (2019) Continuous Erector Spinae Plane Block for Mammary Reconstruction after Mastectomy: Case Report. J Anesth Clin Care 6: 36.
Copyright: © 2019 Vera Lúcia Fernandes de Azevedo, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
© 2026, Copyrights Herald Scholarly Open Access. All Rights Reserved!