General Anesthesia to Low Flows with Sevofluran in Patients of Colecistectomy by Video Laparoscopy, Regional National Hospital San Juan De Dios, San Miguel, year 2019
*Corresponding Author(s):
José Mauricio-AparicioHead Of The Department Of Anesthesiology Of The National Regional Hospital San Juan De Dios Of San M, El Salvador
Tel:+503 71708903,
Email:jmvoc19@yahoo.com
Abstract
Objective: To assess the effectiveness of general anesthesia at low flows with Sevoflurane in patients with Video laparoscopy Cholecystectomy.
Methodology: Parallel clinical trial, 80 patients who met the inclusion criteria were studied, divided into two treatment groups; treatment 1 general anesthesia at low flows with oxygen at 1 lts/min and sevoflurane, and treatment 0 general anesthesia at high flow with oxygen at 3 lts/min and sevoflurane. The degree of humidification and temperature of the inspired gases, the time of recovery of anesthesia, oxygen consumption and sevoflurane per minute of use, and the presence of aesthetic gases in the operating room environment were evaluated. The results were processed through the statistical program SPSS version 25.0, under statistical tests of T Student and U Mann-Whitney. A bilateral statistical significance at a value of p ≤ 0.05 was considered.
Result: The relative humidity and temperature of the inspired gases was higher in the treatment at low flows, from minute 15 with p = 0.000. Oxygen consumption and sevoflurane reflecting, is lower for low flows with p = 0.000. The recovery time of the anesthesia increased by an average of 10 min compared to the high flow group. The presence of anesthetic gases inside the operating room could not be verified by this study.
Conclusion: General anesthesia at low flows with Sevoflurane is effective as the patient receives higher relative humidity and temperature of the inspired gases, in addition to reducing oxygen consumption and sevoflurane.
Keywords
Effectiveness; General anesthesia; Low flows; Sevoflurane; Video laparoscopy cholecystectomy
INTRODUCTION
Aldrete defines the low flows as the administration of gaseous miscellanies, from the immediately low limit of the alveolar ventilation per minute, up to the flow needed only to fulfill the basic consumption of oxygen and the absorption of the anesthetic agent [1].
For the definition of low flows, we owe to help of classifications previously described by Baker, the Simionescu classification and captured later by Baxter in its review of low and minimal flows, which can be observed next: [2]
|
Metabolic flow |
250 mL/min |
|
Minimum flow |
250 to 500 mL/min |
|
Low flows |
500 to 1,000 mL/min |
|
Medium flows |
1 to 2 L/min |
|
High flows |
2 to 4 L/min |
|
Very high flows |
> 4 L/min |
If a smaller flow of fresh gas is established, the anesthetic gases in the patient’s exhaled air are returned through closed or semi-closed re-breathing systems, all of which establishes a series of benefits that can be divided into clinical, economic and ecological [3].
We are immersed in a process of globalization where the role of the anesthetist must be that of a great planner, using strategies in decision-making to reduce costs and maximize the benefits of anesthetic procedures, it is for this reason that anesthesia at low movements have taken a strong resurgence in recent years, due to clinical, economic, ecological factors and modernization in monitoring technology. Thus, with the arrival of different modern anesthesia machines in the environment, the availability of complete monitoring of anesthetic gases and vapors, the constant use of advantageous but expensive inhaling agents such as sevoflurane and due to the limitation in the use of Health resources, especially in developing countries such as El Salvador, is that this study aims to obtain evidence-based information on the difficulty of general anesthesia at low levels with Sevoflurane in Video laparoscopic Cholecystectomy patients at the Regional National Hospital “San Juan de Dios”, San Miguel.
MATERIALS AND METHODS
A study was carried out, which by design is a controlled, randomized clinical trial, with parallel groups, the sampling technique was of simple random type, 80 patients were included: men and women, ASA I and II, undergoing celectoscopic cholecystectomy, under balanced general anesthesia, between 18 and 60 years old and BMI between 18.5 and 30 kg/m2, with surgical time < 2 hrs and who signed the informed consent (Figure 1).
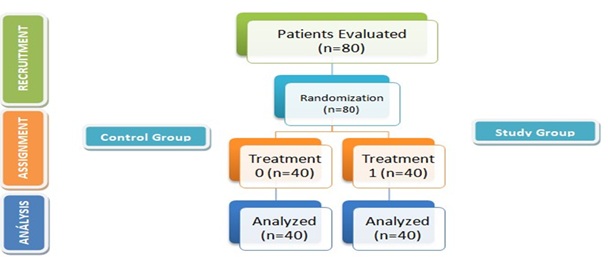
Figure 1: Flowchart of randomized clinical trial.
Two groups were defined: treatment 1: general anesthesia at low oxygen flow (1 L/min) with sevoflurane. Pre-oxygenation with nasal cannulae is performed at 5 Lts/min FiO2. 40% for 3 minutes, at the same time, a pre-filling of the circular circuit with the overpressure technique with a flow of O2 5 L/min and sevoflurane 8 Vol% for 3 min. After that time Atropine 0.5 mg IV is administered as standard dose and propofol 50 mg IV plus positive pressure ventilation with face mask with a flow of O2 5 L/min and sevoflurane 8 vol%, when the patient loses consciousness, fentanyl is administered at a dose of 2 µg/kg, propofol 2.5 mg/kg, succinylcholine 2 mg/kg IV, laryngoscopy and orotracheal intubation. The patient is connected to mechanical ventilation and administered of cisatracurium at dose 0.1 mg/kg IV.
When the patient reaches the target MAC value 1.0 - 1.25, the flow with 100% oxygen is reduced to 1.0 L/min and the vaporizer dial is changed between values of 3 to 5 Vol%.
Prior to the end of the procedure, a reduction to the vaporizer agent is performed to 0% approximately 10 minutes before the end of surgery, where oxygen flow is maintained at 1 liter per minute until the patient begins to have a pattern respiratory. The patient is transitioned to spontaneous breathing with 100% oxygen at 6 liters per minute and will be maintained until the patient meets the extubation criteria.
Treatment 0: general anesthesia at high oxygen flows (3 L/min) with sevoflurane. Pre-oxygenation and induction similar to treatment group 1 and after connecting the patient to mechanical ventilation and administration of cisatracurium is adjusted the flow of fresh gas with 100% oxygen to 3 L/min and the dial of the sevoflurane vaporizer is placed between 2 - 2.5 Vol%, keeping a MAC between 1.0 - 1.25.
Prior to the end of the procedure, a reduction to the vaporizer agent is performed to 0% approximately 10 minutes before the end of surgery, where oxygen flow is maintained at 1 liter per minute until the patient begins to have a pattern respiratory. The patient is transitioned to spontaneous breathing with 100% oxygen at 6 liters per minute and will be maintained until the patient meets the extubation criteria.
For both groups, at the end of the anesthetic procedure a 50cc sample of ambient air from the operating room was taken and passed through the gas analyzer of the Mindray A5 anesthesia machine.
It was recorded by the observation guide, the relative humidity in %, and the temperature of the gases inspired by every 5 minutes, the amount of O2 used and the vol% on the sevoflurane dial every 3 minutes, at the close of the sevoflurane vaporizer dial, the recovery of anesthesia was recorded by the modified Aldrete scale every 5 minutes and a note 8 was instituted as a recovery value, environmental pollution expressed in MAC value at the end of the anesthetic procedure, and sevoflurane consumption is defined by the use of the following formulations:
Formulation 1
Anesthetic vapor volume = (%) anesthetic X (fresh gas flow / 100 - (%) anesthetic)
Formulation 2
Liquid volume = Volume of steam used / Vapor produced per ml of anesthetic.
In each ml of liquid sevoflurane there are 182.7 ml of anesthetic vapor [4].
The statistical analysis was carried out using the SPSS v 25.0 program, after obtaining the data, the Shapiro-Wilk normal test was performed, the data group to which a normal distribution was determined was performed the statistical test of t-student, and when the U Mann-Whitney test was obtained, and a bilateral significance with a value of p ≤ 0.05 was considered.
RESULTS
A total of 80 patients were studied: n = 40 (50%) treatment group 0, n = 40 (50%) treatment group 1, with an average age of 38.68 ± 12.08 for treatment 0 and 35.80 ± 12.36 for treatment 1, I predominance the female sex for both treatment groups 55% and 60%, and a physical stage ASA I 70% and 62.5% respectively (Table 1).
|
Groups |
Treatment 1 N = 40 |
Treatment 0 N = 40 |
|
Age |
38.68 ± 12.08 22/59 |
35.80 ± 12.36 22/59 |
|
Weight |
72.56 ± 9.87 50.0/91.6 |
69.76 ± 9.52 50.0/92.0 |
|
Size |
164.50 ± 8.92 148.0/180.0 |
169.02 ± 9.34 148.0/182.0 |
|
BMI |
26.65 ± 2.09 22.22/29.79 |
25.99 ± 2.31 22.00/29.72 |
|
Sex (M/F) |
45.0% (18) / 55.0% (22) |
40.0% (16) / 60.0% (24) |
|
ASA (I Y II) |
70.0% (28) / 30.0% (12) |
62.5% (25) / 37.5% (15) |
Table 1: General Data.
The moisture and the temperature of the inspired gases increases from 15 min in the anesthesia low flows, with a bilateral significance of p = 0.000, obtaining the registered maximum average of relative moisture for the treatment 1 of 98.20 ± 1.476 % to 105 min and of 61.59 ± 11.554 % to 90 min for the treatment 0, as for the temperature, the biggest registered one was 25.960 ± 1.1436 °C to 75 min for the treatment 1 and 24.172 ± 0.7911 °C to 60 min, for the treatment 0, with a bilateral significance of p = 0.000 (Figures 2 and 3).
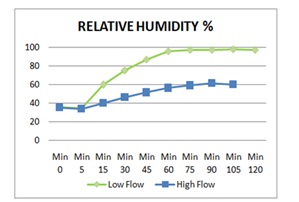
Figure 2: Relative humidity of inspired gas.
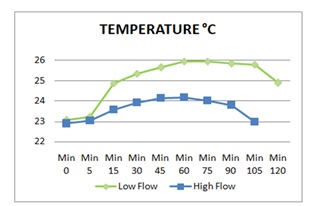
Figure 3: Temperature of inspired gas.
The time of use of sevoflurane had an average of 69.30 ± 17.393 min for the group 1 and 72.72 ± 17.653 min for the group 0, with a bilateral significance of p = 0.382, and the time of use of oxygen was 90.77 ± 17.483 min for the treatment 1 and for the treatment 0, 87.45 ± 17.445 min with a bilateral significance of p = 0.452.
The sevoflurane consumption had an average for the treatment 1, 16.55 ± 2.084 ml and for the treatment 0, 33.02 ±
6.415 ml, with a bilateral significance of p=0.000, and the time of consumption of oxygen was to 148.85 ± 18.520 L, for the treatment 1 and 295.12 ± 59.927 L for the treatment 0, with a bilateral significance of p=0.000 (Figures 4 and 5).
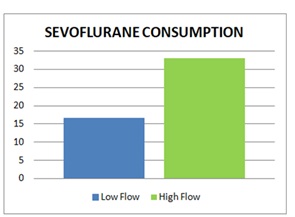
Figure 4: Consumption of sevoflurane in ml.
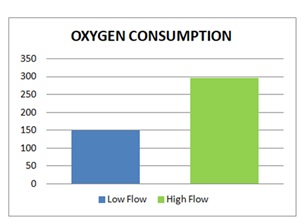
Figure 5: Oxygen consumption in L.
The time of recovery of the anesthesia in which a note bigger than 8 was obtained in the modified Aldrete scale was to 20 min in the group of treatment 1, with an average of 9.89 ± 1.811 and for the group 0 to 10 min with an average of 8.85 ± 1.833 (Figure 6).
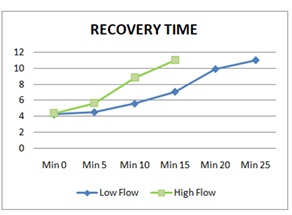
Figure 6: Anesthesia recovery time.
As for the recording of environmental pollution, no data were obtained.
DISCUSSION
The patients with mechanical ventilation lose the functions of the top airway, of warming and humidification of the inspired gases [5]. On having been ventilated by dry and cold gases, they present a continuous loss of moisture and heat that it predisposes to complications of the airway, such as: alterations of the mucociliary transport, thickening of secretions, dyskinesia ciliary and desquamation epithelial, which drives to hypothermia, hypoxemia and atelectasias to avoid these complications, the patients submitted to anesthetic procedures with intubation endotracheal it is necessary to provide gases with a relative moisture of between 95 - 100 % and a temperature between the status from 28 to 34 °C [6,7].
José S, et al., in 2017 perform a meta-analysis on the effects of different flows of fresh gas with or without a heat and humidity exchanger on the humidity of inhaled gas in adults under general anesthesia, the results have concluded that a higher humidity of the inspired gases is obtained using low flows, in comparison with the high flows with IC 95%: 4, 53 a 9, 86; p < 0,001 [8].
The results of our study imply that general anesthesia and low flows contribute to increase the humidity and temperature of inspired gases, as described in the literature, reducing the implicit complications of an artificial airway.
Ho-Geol Ryu, et al., implemented a low flow policy in 2011 (1 L/min) by increasing the number of anesthetic hours per sevoflurane bottle from 250 ml to 10.5 hours per bottle to 17.4 hours, with an increase of 73.7%. Gaston M, et al., in 2008 found that the amount of liquid halothane used went from 20 ml per hour, to 7.68 ml ± 0.58 for the first hour, and from 5.25 ml for the second hour of surgery in procedures that lasted more than one hour, with the use of low flows (1 L/min) [9,10].
As for the recovery time of anesthesia, this is higher in anesthesia at low flows, despite that the consumption of oxygen and sevoflurane is not increased due to these factors, Checking as described by Christian Hönemann BM Low flow anesthesia, minimum flow and metabolic flow “clinical techniques for use with reinhalation system”, in 2004 [11].
Our investigation showed that oxygen consumption is reduced by 50% and in the case of sevoflurane in anesthesia at low flows, 18.11 hours of anesthesia per 250ml bottle occurs, contrary to the control group, where 9.26 hours per bottle occurs.
In the case of environmental pollution, the research group did not have the specific equipment to measure the presence of anesthetic gases in the operating room, so it was not possible to record data and check this variable, despite this, there is a lot of theory which supports that the use of anesthesia at low flows reduces the presence of anesthetic agents, such as that performed by Leonardo A., in 2001 where he demonstrated a reduction in the amount of isoflurane removed to the operating room, of 1.26 MAC ( with 4 L/min), at 0.72 MAC (with 1 L/min) and at 0.46 MAC (with 0.5 L/min). When the flow was reduced from 4 to 1 and from 4 to 0.5 L/min, the elimination fell to 56.7% and 36.2%, with a decrease in pollution of 43.3% and 63.8% respectively [12].
CONCLUSION
At the end of the research topic, we declared as a study group that we have no conflicts of interest, economic, institutional, work or personal.
It is concluded that general anesthesia at low flows with sevoflurane is effective in patients with video laparoscopic cholecystectomy, San Miguel de Dios Regional National Hospital in San Miguel, since it provides a higher relative humidity and temperature of the inspired gases, than in the general anesthesia at low flows with sevoflurane, the time to wake up post-anesthetic is longer, a lower consumption of oxygen and sevoflurane was demonstrated by anesthetic procedure when using anesthesia at low flows, achieving economic savings, and With respect to anesthetic risk, it is demonstrated that it is a safe technique, similar in safety to general anesthesia at high flows; not having trans or post- anesthetic morbi-mortality, in both treatment groups.
REFERENCES
- Aldrete JA (2004) THEORETICAL-PRACTICAL ANESTHESIOLOGY TEXT. Editorial El Manual Moderno, Mexico, 970-729-059-5.
- Portela-Ortiz JM, Hernández-Cortés C, Delgadillo-Arauz DC (2015) Low Flows in Anesthesia. Mexican Journal of Anesthesiology 38: 352-355.
- Baum JA (1995) Low-flow anaesthesia. Anaesthesia. 50: 37-44.
- Laster MJ, Fang Z, Eger EI (1994) Specific gravities of desflurane, enflurane, halothamo, isoflurane, amd sevoflurane. Anesth Analg 78: 1152-1153.
- Sylvester J, Konstantatos A (2017) Humidity in Anesthesia. Anaesthesia Tutorial of the Week Page no: 1-4.
- Hernández-Jiménez C,Olmos-Zuñiga JR, García-Torrentera R, Jasso R, Solís-Bravo T, et al. (2011) Effects of gas humidification tion on mechanical ventilation: An experimental study. Revista del Instituto Nacional de Enfermedades Respiratorias 70: 247-251.
- Parisoto A (2003) Patient care with mechanical respiratory assistance. IntraMed.
- Braz JRC, Braz MG, Hayashi Y, Martins RHG, Betini M, et al. (2017) Effects of different fresh gas flows with or without a heat and moisture exchanger on inhaled gas humidity in adults undergoing general anaesthesia: A systematic review and meta-analysis of randomized controlled trials. Eur J Anaesthesiol 34: 515-525.
- Ryu HG, Lee JH, Lee KK, Gil NS, Kim CS, et al. (2011) The effect of low fresh gas flow rate on sevoflurane consumption. Korean J Anesthesiol 60: 75-77.
- Gastón M, et al. (2009) Balanced General Anesthesia with Low Flows. Cochabamba: Bolivian Medical Gazette, 32: 1012-2966.
- Hönemann C, Mierke B (2004) Low Flow, Minimum Flow and Metabolic Flow Anesthesia: Clinical techniques for use with reinhalation systems. Dräger, Lübeck, Germany.
- Cost of general anesthesia with high, medium, low and minimal flows. Comparative Study. Guillermo Almenara Irigoyen National Hospital. L., Candle. Peru. Lima: s.n.
Citation: Mauricio-Aparicio J, Luis-Quitoc M, María-Amayad E, Balmore-Chávezd I, Milagro-Castilloc J (2020) General Anesthesia to Low Flows with Sevofluran in Patients of Colecistectomy by Video Laparoscopy, Regional National Hospital San Juan De Dios, San Miguel, year 2019. J Anesth Clin Care 7: 049.
Copyright: © 2020 José Mauricio-Aparicio, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.