Langerhans Cell Histiocytosis of Thoracic Vertebra in an Adult: A Case Report and Review of the Literature
*Corresponding Author(s):
Nilgun KatranciDepartment Of Nursing, Gaziantep University, Sahinbey, Turkey
Tel:+90 3423606060,
Email:nilselgun@hotmail.com
Abstract
Since there is not a standard treatment for patients with multisystem complaints, presenting more cases with this disease will have a great contribution.
ABSTRACT
Keywords
INTRODUCTION
LCH is a rare disease characterized with abnormal proliferation of histiocytes originated from bone narrow with an unknown etiology [1]. It is usually seen in the pediatric age group and defined in three different ways as Eosinopholic Granuloma, Hand Schuller Christian and Letteree-Siwe according to clinical and pathological characteristics [2]. The disease can be local or systemic and involvement can be seen mostly in skin, bone, lymph nodes, lungs and central nervous systems. Men are affected more often than women [3].
CASE REPORT
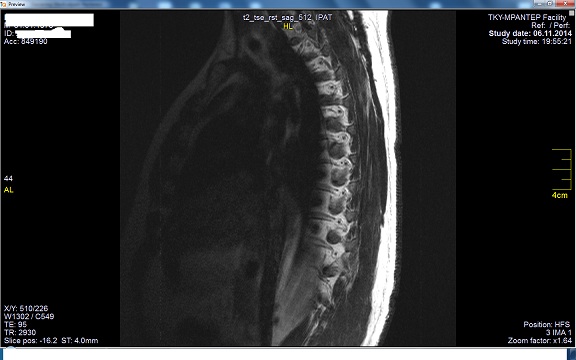
Figure 1: Thorocal MR.

| Drugs | Drug Application Methods | 1st Day | 2nd Day | 3rd Day | 4th Day | 5th Day | 6th Day | 7th Day |
| Prednol 40 mg/m² | Oral | + | + | + | + | + | + | + |
| Vinblastine 6 mg/m² | I.V. Push | + | ||||||
| Osteovita | Oral | + | + | + | + | + | + ..For 12 days |
Table 1: Treatment Protocol.
After three months of treatment, significant regression was seen in the patient and the treatment protocol created again, he received Vinblastine 12 mg every month, Prednol 80 mg for 5 days from the date of administration Vinblastine and 6-mercaptopurine 100 mg every day for 12 months as the follow-up treatment. During this period, the patient was checked every 3 months and no tumoral symptoms or recurrence was observed. A full recovery was seen. The patient was smoking 1 pack a day before being diagnosed with LCH. Despite recommendations, he didn't quit smoking during treatment (Figure 1).
DISCUSSION
LCH is considered to be a pediatric disease and it is estimated annual prevalence of 1 case per 560,000 in adults [4]. its etiology is not yet known and it is still controversial whether it is a neoplastic process or an atypical immunological reaction [5]. According to the studies conducted, the recent findings towards mutation of BRAF [6] and MAP2K1 [7] suggest that the disease has a neoplastic origin [5].
It is reported that the diagnosis of LCH is sometimes difficult and it can be diagnosed lately or even be unnoticed in the adult population in particular [1,5]. Although PET-BT application is useful in the diagnosis, it has been reported to be insufficient to establish a final diagnosis [8]. There are not any symptoms, physical examinations or laboratory findings that are specific to the disease, and it is diagnosed by immunohistochemical analysis. The definitive diagnosis is obtained by showing the Langerhans cells stained with S-100 and CD1a antigen in the biopsy [9,10]. These cells are mostly eosinophils, leukocytes, neutrophil leukocytes, lymphocytes or plasma cells [10].
Three different clinical forms have been described as Eosinopholic Granuloma (EG), Hand Schuller Christ?an and Letteree-Siwe. EG is characterized by either a single or a large number of bone lesions and it can involve all the bones, especially the skull and it is mostly reported to be involved in pelvis and ribs [11]. Hand Schuller Christ?an and Letteree-Siwe are more aggressive forms that holds in visceral organs such as lung, liver and skin. The single organ involvement is reported as second skin after bone involvement [14]. Isolated skin LCH has a good prognosis in general, however reactivation in the skin or progression to the disseminated, sometimes fatal, form can also occur [1].
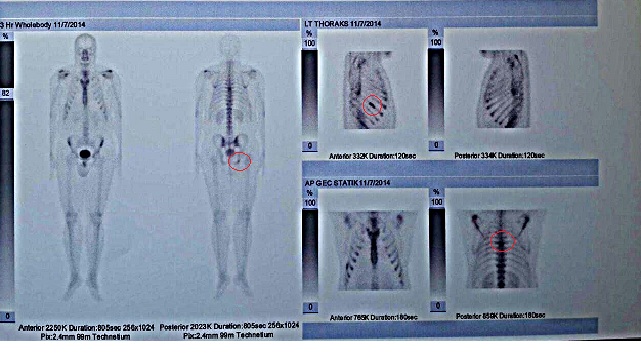
In our case, due to the complaints of the patient, thoracic MRI scan was performed and contrasting patterns were observed in the T6 vertebra corpus, T12 vertebra inferior in a smaller size and in the level of spinal cord right postero lateral segment on the level of T7-8 disc in millimeter-level. According to the bone scan results, suggested the metastatic spread of a malignant process; thus, PET-BT is proposed to be used for further evaluation. Reconstructive surgery applications are recommended in large bone defects [12]. Due to advanced defects in vertebrae, spinal tumor ablation was applied on our patient and the diagnosis was clarified by the pathology results.
Treatment of LCH varies depending on whether the disease is localized or widespread and the surgery, radiotherapy, local and systemic steroid therapy and chemotherapy may be used [13]. LCH is examined in two groups as a single system or multisystem involvement depending on the organ involvement [9,14,15]. In our patient, LCH was diagnosed by the pathology received from liver outside the thoracic vertebrae. According to the LCH classification, the patient was considered to be in the high risk group since he had multisystem involvement. Patients with multisystem involvement are recommended to receive combined treatments and they usually receive both systemic chemotherapy and systemic steroid therapy [9,15]. Due to the lack of a wide range of treatment models in the literature, different treatment models are applied in different centers. Inci et al. have observed a significant regression in a patient with lung and bone involvement after applying 12 mg/week i.v. Vinblastine, 80 mg/ day Metilprednizolol, 100 mg/ day 6-merkaptopürin for 3 months [9]. It is similar to our patient treatment plan in this review.
CONCLUSION
In this study, diagnosis and treatment of LCH disease in thoracic vertebrae and soft tissues of adult patient was presented. LCH is a rare disease of unknown etiology. Radiological tests help in its finding and immunohistochemical analysis are confirmatory. LCH syndromes have a relatively bening course in adult patients and treatment has got good results. Due to it is a rarely seen and not well-defined disease in adults, LCH may be considered as a differential diagnosis in patients with osteolytic bone lesions. Since there is not a standard treatment for patients with multisystem complaints, presenting more cases with this disease will have a great contribution.
CONFLICT OF INTEREST
The author(s) declare no potential conflicts of interest, with respect to the research, authorship, and/or publication of this article.
REFERENCES
- Abla O, Egeler RM, Weitzman S (2010) Langerhans cell histiocytosis: Current concepts and treatments. Cancer Treat Rev 36: 354-359.
- Broadbent V, Egeler RM, Nesbit ME Jr (1994) Langerhans cell histiocytosis--clinical and epidemiological aspects. Br J Cancer Suppl 23: S11-16.
- Sahin F, Ozen KP, Vural F, Kamer S, Arg?n M, et al. (2007) Retrospective analysis of seven patients with adult-onset Langerhans cell Histiocytosis syndromes: A single center experience. Turk J Hematol 24: 75-79.
- Wang S, Zhang W, Na S, Zhang L, Lang Z (2014) Langerhans cell histiocytosis of the clavicle: a case report and review of the literature. Medicine (Baltimore) 93: 117.
- Udaka T, Susa M, Kikuta K, Nishimoto K, Horiuchi K, et al. (2015) Langerhans Cell Histiocytosis of the Clavicle in an Adult: A Case Report and Review of the Literature. Case Rep Oncol 8: 426-431.
- Badalian-Very G, Vergilio JA, Degar BA, MacConaill LE, Brandner B, et al. (2010) Recurrent BRAF mutations in Langerhans cell histiocytosis. Blood 116: 1919-1923.
- Brown NA, Furtado LV, Betz BL, Kiel MJ, Weigelin HC, et al. (2014) High prevalence of somatic MAP2K1 mutations in BRAF V600E-negative Langerhans cell histiocytosis. Blood 124: 1655-1658.
- Phillips M, Allen C, Gerson P, McClain K (2009) Comparison of FDG-PET scans to conventional radiography and bone scans in management of Langerhans cell histiocytosis. Pediatr Blood Cancer 52: 97-101.
- ?nci R, Sayar H, ?nci MF, Öztürk P (2014) Adult Onset Langerhans' Cell Histiocytosis. Turk J Dermatol 4: 236-239.
- TUN K, TÜRKO?LU OF, OKUTAN O, YE??LKILIÇ S, BE?KONAKLI E (2005) Eosinophilic Granuloma in the Young Adult Patient: A Case Report. J Neurol Sci (Turk) 22.
- Islinger RB, Kuklo TR, Owens BD, Horan PJ, Choma TJ, et al. (2000) Langerhans' cell histiocytosis in patients older than 21 years. Clin Orthop Relat Res: 231-235.
- Basmaci M, Hastürk AE (2011) Eosinophilic Granuloma: Radiological and Clinical Evaluation. Turk Nörosirürji Derg. 21: 262-264.
- Ç?L T, GÖKALP D, TUZCU A, I?IKDO?AN A, BAHÇEC? M (2007) Adult Langerhans Cell Histiocytosis: Differential Diagnosis. Türkiye Klinikleri J Med Sci 27:633-635.
- Campanati A, Simonetti O, Marconi B, Giuliodori K, Ganzetti G, et al. (2009) Purely cutaneous Langerhans' cell histiocytosis in an adult woman. Acta Derm Venereol 89: 299-301.
- SERDAR ZA, G?ZENT? S, YA?AR S, GÖNENÇ I, GÜNE? P (2012) Adult Onset Langerhans' Cell Histiocytosis: A Case Report. Marmara Medical Journal 25: 96-99.
Citation: Citation: Katranci N, Sharma S (2017) Langerhans Cell Histiocytosis of Thoracic Vertebra in an Adult: A Case Report and Review of the Literature. J Cancer Biol Treat 4: 010.
Copyright: © 2017 Nilgun Katranci, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.