Prognosis Scores of Extracorporeal Membrane Oxygenation and Programming of a ECMO Database
*Corresponding Author(s):
Vera Von DossowInstitute Of Anaesthesiology, Heart And Diabetes Center Bad Oeynhausen, Ruhr-Universität Bochum, Germany
Tel:+49 5731 971128,
Fax:+49 5731 972196
Email:vvondossow@hdz-nrw.de
Abstract
Extracorporeal Membrane Oxygenation (ECMO) is increasingly being utilized as a life support for severe respiratory and/or cardiac failure refractory to conventional treatments. For a reasonable risk stratification, several outcome prediction scores were developed to estimate the survival probability of ECMO patients. In the practical part of the underlying project, an extensive ECMO database in form of a web application consisting of 13 different forms made up of graphical control elements was programmed using Python on behalf of a particular health care institution. The aim of this study was to investigate outcome prediction factors of two selected scoring systems and to impart information about the programming of a database application. Age, duration of intubation or mechanical ventilation prior to ECMO, immunosuppression, weight, haemodynamic and respiratory parameters, application of drugs, diagnosis groups and associated complications are among the influencing factors that either have a positive or negative impact on the outcome and are used to predict the survival chances of ECMO patients. It can be concluded that risk factors outnumber protective factors and that the accuracy of the scores may be considered as questionable due to the complex nature of the issue and the abundance of unpredictable factors. With the database, a sustainable contribution to optimize procedures can be achieved.
Keywords
Database; Extracorporeal membrane oxygenation; Outcome prediction scores
INTRODUCTION
In the past few decades, the use of Extracorporeal Membrane Oxygenation (ECMO) in intensive care medicine has grown exponentially. Extracorporeal life support has advanced to an important treatment for severe respiratory and/or cardiac failure that is refractory to conventional rescue treatments [1]. It targets critically ill patients who would otherwise face a grim prognosis with a high mortality rate [2]. A life support circuit which includes a membrane oxygenator in either venovenous or venoarterial configuration is implanted to assist respiratory and occasionally cardiac function [3]. The outcome of this technique has improved steadily over time as a result of better equipment and greater experience. The number of patients treated with ECMO increases continuously which raises new ethical questions about when to initiate or terminate extracorporeal life support [4].
Although this treatment could save the lives of critically ill patients, it is still accompanied by a relatively high rate of complications. Therefore, a careful risk-benefit analysis must be conducted to select the patients who would most likely benefit from ECMO. The survival rate varies depending most notably on the indication, patient group and ECMO center. In total, it amounts to about 50 to 60 percent [5].
For a reasonable risk stratification, outcome prediction scores were developed to estimate the chances of survival of ECMO patients. The basis of these scoring systems are forms built up of graphical control elements with certain parameters. Each parameter is assigned a positive or negative score. Items with a positive score are protective factors which are believed of increasing the chances of survival, those with negative scores are risk factors that can be linked to a worse outcome. The scores are added to a total score that in turn gives an approximation of the survival probability in percent.
In the treatment of ECMO patients, an individual severity assessment through scoring systems could be used to estimate the survival probability of potential candidates for ECMO, to inform relatives about the condition of the patient and to enable a risk-adjusted comparison of outcomes between centers [6]. Additionally, ECMO demands a high amount of human and financial resources. Hence, a rational allocation of these limited resources is also of great importance [7].
The Extracorporeal Life Organization (ELSO) is an international non-profit consortium of health care institutions. Its aim is to maintain a registry of extracorporeal membrane oxygenation use in ELSO centers. Another mission is to sustain guidelines regarding the application of ECMO. Today, over 350 centers worldwide are ELSO members and have together reported over 65000 ECMO treatments [8].
Inspired by the ELSO database, a similar database for a particular hospital should be built up to collect and save all data regarding the application of ECMO in this health care institution. Firstly, a prototype was programmed that in the next step has to be integrated into the clinic´s own system. This database application consists of a total of 13 web forms made up of different graphical control elements in which the parameters are sorted by topic. The forms include parameters that are included in the ELSO database as well as specially defined parameters. Built-in interactive functions and features were integrated to facilitate operations. Most databases, including the present one, are relational databases. These are composed of tables through which all accesses are conducted. All tables are connected via relations which are saved in the tables [9]. Besides selection and search functions, the programmed database must also enable management functions [10].
Despite the vast expansion of extracorporeal life support, some outcome factors have not yet frequently been studied. The objective of this paper is to impart a better understanding of outcome prognosis factors and the programming of a database application.
We hypothesized that the analysis of prognosis factors and the programming of a database would optimize procedures and organization of ECMO in this particular health care center.
MATERIALS AND METHODS
The database application was programmed using Python as programming language. It was created within the scope of a web framework named Django. A framework covers by definition all software components that provide an application architecture. In addition, JavaScript was utilized to program certain functions as well as the markup language HTML to create the front-end-part of the application.
Each of the 13 forms deals with a different topic. The overview page contains the basic information of the patients treated. The first form to be filled out is the admission form. It includes the demographic data regarding the admission and ECMO configuration. The Pre-ECMO form holds facts surrounding intubation as well as ventilator settings and haemodynamic parameters. The transport form contains data of an eventually performed transportation on ECMO. The indication form carries information about the indication for ECMO, blood gases and catecholamins. The daily base form contains data of daily performed procedures, laboratory results and infectious organisms. A form named cardiac supplementary form collects information about pre-, inter- and post-operative echocardiography. The implantation form includes data about the equipment that is used for ECMO runs. The Pediatric/Neonatal form contains special information surrounding the use of ECMO on infants and children. Moreover, the complications are registered by an own form made up of checkboxes. The ECPR supplementary form, Weaning/Explantation form and change of configuration form include data about the topic the form is named after. Lastly, the epicrisis form holds facts about the outcome of the treatment.
Two different prognosis scoring systems were analyzed which can be retrieved on the official ELSO website. The RESP Score (Respiratory ECMO Survival Prediction Score) gives an estimation of the survival rate for adult ECMO patients with respiratory failure. The SAVE Score (Survival After Veno-arterial ECMO) approximates the survival rate of patients undergoing VA-ECMO. Both appear as forms with radio buttons and toggles as graphical control elements. The RESP score ranges from a total score of -22 to 15, the SAVE score from a score of -35 to 17. A higher score corresponds to a better survival rate and a score of 0 approximates to a survival rate of 50 percent.
The RESP score is built up of following items as prognosis factors: age, immunocompromised status, duration of mechanical ventilation prior to ECMO, acute respiratory diagnosis group, central nervous system dysfunction, acute associated (nonpulmonary) infection, neuromuscular blockade agents before ECMO, Bicarbonate infusion before ECMO, nitric oxide use before ECMO, cardiac arrest prior to ECMO, PaCO2 (carbon dioxide partial pressure) and peak inspiratory pressure.
The SAVE Score consists of the following prognosis factors: acute cardiogenic diagnosis group, age, weight, acute pre-ECMO organ failures (liver failure, central nervous system dysfunction, renal failure), chronic renal failure, duration of intubation prior to initiation of ECMO, peak inspiratory pressure, pre-ECMO cardiac arrest, diastolic blood pressure before ECMO, Bicarbonate prior to ECMO and a constant value of -6 to added to all calculations.
RESULTS
To program a form that is connected to a database, several steps need to be passed through. In this part, the components of the database application as well as important operational steps and background information are explained. Additionally, the structure of the forms are described and additional features are outlined. Django as a web framework follows a specific software design pattern that all modern web frameworks have in common. In this case, the application is based on the so-called MTV model that consists of the three components model, template and view. The model defines the structure of the data and also provides the interface to the underlying database, the template is the part of the application seen by the user and the view acts as a link between model and template [11].
A database application generally consists of two components, the front-end and the back-end. The front-end represents the graphical User Interface (GUI) and illustrates the data seen by the user. The back-end is the database itself which manages the data automatically in the background.
A model can be described as a single, definitive source of information of the data saved [12]. It includes the fields and behavior of the data that is being stored. This part of the application is made up of several classes and subclasses that each represent a table in the database. Every class contains a specific number of fields that each correspond to a column in the tables. In accordance with the classes in the models, objects are created and saved in the views. The classes and thus the tables are connected via foreign keys which also enable an interaction between the tables.
In a web framework, there must be a practical way to generate HTML (Hypertext Markup Language) dynamically. The templates are as opposed to other components of the program written in the markup language HTML. A template contains both the static part of the desired HTML output and the special syntax of how the dynamic content is inserted. Templates are practically simple text files that support and display every text-based format such as HTML, XML and CSV. A template consists of variables that are replaced by a value as well as tags that illustrate the logic of the templates and manage their control flow [13].
Besides pure navigating on the website, interactive web applications must have advanced functionalities. In this project, it includes the submission of form data, its processing and subsequent deposit in the database. For this function, technical requirements must be fulfilled. The data entered by the user needs to be handed over to the application server through an interface. In this context, the Hypertext Transfer Protocol (HTTP) offers two possibilities of argument transfer: GET and POST [14]. In general, the HTTP serves as a communicator between client and server. The function GET requests data from a specified source, the other method POST submits data that is processed to a stated resource [15]. Both GET and POST work with HTML forms as mediator that connect the named placeholders with the data [14].
Loading and accessing a form takes place in a certain way. When a site is requested, Django creates a http Request object that contains the metadata of the request. Subsequently, Django loads the corresponding view. Every view is responsible for returning an answer in form of a httpResponse object [16]. All objects that are handed over are packed in the so-called context. A context is in general a series of variable names and their values. A template uses these to fill their variables and to evaluate their tags[13].
The Graphical User Interface (GUI) determines the appearance of the site. These are built up of windows with different graphical control elements, also called widgets. The most common widget in the forms is a simple text field. Further graphical control elements are number fields, date and time fields in their typical format, checkboxes, radio buttons and drop-down-menus. Checkboxes which have a quadratic form and radio buttons which have a round form can each take up one of two possible states, either activated or deactivated. In a group of interrelated items, none up to all checkboxes can be selected independently whereas with radio buttons, only exactly one item can be selected and thus activated. Drop-down-menus have the same function as radio buttons and allow a better overview when there are multiple selectable items. At the end of the forms, there are two buttons to confirm and send the form that has just been filled out and to return to the main page.
JavaScript is one of the widespread script languages that allows among other aspects to build in interactive functions in a website. In general, it is used to design and to control the behavior of a website in an event-controlled matter [17]. In this project, JavaScript was utilized to manage the behavior of checkboxes and radio buttons instantaneously through simple clicking on the buttons. This is done by integrating JavaScript in the HTML code. Firstly, all elements needed for a certain function are collected in an array, followed by additional details. Under the usage of boolean variables, the behavior of the checkboxes or radio buttons are controlled depending if it is the first or second click on the button. This as well as the type of graphical control element causes different actions. The function checks each parameter if it is activated or deactivated. Several constellations are covered by the function. This includes a checkbox placed in front of a text field which is activated by a click on the checkbox, to intercept missing information and to activate or deactivate a group of interrelated fields.
In the database, another feature is integrated that calculates certain parameters automatically including necessary unit conversions using the data entered by the user. This includes the BMI (Body Mass Index), BSA (Body Surface Area), IBW (Ideal Body Weight) and ABW (Adjusted Body Weight) with generally valid formulas. The age is calculated by cutting out parts of a string and then subtracting the birth date from the current date. Similarly, the ECMO running time is computed by subtracting the date of the installation of ECMO from the current date. In all cases, the results were rounded to a clear value.
The functionalities of the database can be expanded with further innovative functions. The static insertion of contents can be connected to dynamic functionalities. For example, while filling out the forms, it is possible to program a function that evaluates and gives a prediction of the entered parameters instantly. Also, after completing a form, an instant analysis of the entered data based on SQL could be built in. Another possibility is to arrange a graphical display on a tablet using webgraph or jqueryUI. Furthermore, an XML interface can be programmed. This links the database to Microsoft Excel and allows an import of laboratory data under the usage of an import function (Figure 1).
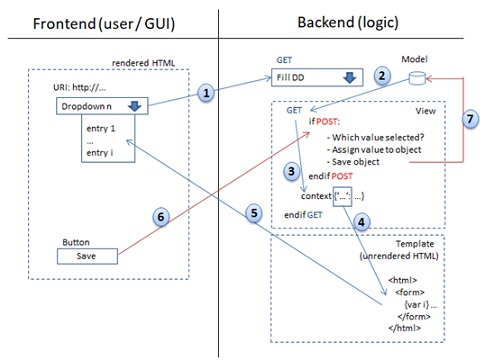
Figure 1: Overview of the programming steps.
The user is presented with the frontend (GUI: graphical user interface) when calling up the URI (uniform resource identifier) in the web browser. After requesting the site through the entry of the URI/URL, the backend is prompted via GET command to display the website and for this purpose to create the HTML dynamically, for example via variables that are filled out by the business logic or database before they are returned to the frontend. In this example, a dropdown menu is filled out with values. After giving up the GET command (1) these are retrieved from the database (2) and via the context function (3) handed over to the template (4). These are rendered and the dropdown is filled out with values (5). When a user hereupon selects one of these entries in the rendered HTML of the user interface and clicks on the “save“ button (6), the POST-branch is passed through in the backend (view) which requests the selected value. This is allocated to the object that is deposited in models.py and connected to the database. The object is then linked to the current user and saved in the sqlLite database (7).
DISCUSSION
The outcome is determined by a complex interaction between several influencing factors which are also capable of influencing one another mutually. The most important prognostic factors of the scoring systems are shown in figure 2. Protective factors equal to a positive score, risk factors have a negative score. Some particular factors like age can either have a positive or negative influence on the prognosis depending on the manifestation or reference value.
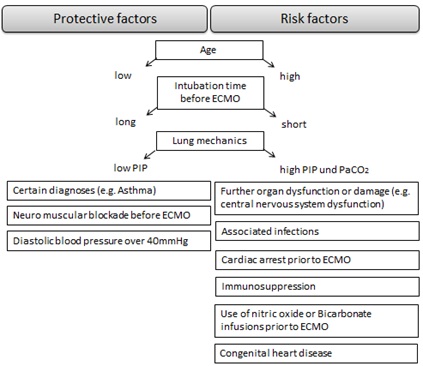
Figure 2: Outcome prediction factors for ECMO.
The age can be considered as a major predictive factor for the survival probability of ECMO patients and is thus represented in both scoring systems. In the RESP Score, a negative value of -2 (ages 50-59) or -3 (age 60 and above) is added to the total score. In the SAVE Score, a young age (18-38 years) has the highest positive score of 7 of all items and thus increases the survival probability drastically. In both scores, the survival probability drops disproportionately from an age of around 60 and above. The scores clearly indicate that in regard to ECMO, a high age is a risk factor that limits the chances of survival and is associated with a significantly higher mortality. Thus, lower success rates must be assumed. This can be backed up with previous studies to this topic and the ELSO guidelines [18-19]. However, an absolute age limit for ECMO is not defined in the ELSO guidelines which means that a therapeutic attempt in senior patients is potentially justifiable if there is a sufficient recovery potential. For newborns and/or children, other specially designed scoring systems are used. The scoring systems also highlight the differences of ECMO application in the various age groups.
In the RESP Score, an immunosuppression is categorized as a risk factor and equals to a score of -2. For instance, complications like infections are seen more often in immunosupprimised patients. These possible complications could be in turn risk factors with a negative impact on the outcome. This could lead to an additive effect of negative factors which can worsen the outcome significantly.
The weight is another demographic parameter incorporated in the SAVE Score. According to this scoring system, a weight below 90 kilograms has a positive score of either 1 or 2 which means that it is assumed to have a positive impact on the prognosis. This however contradicts other studies about this topic. In a study of Cho et al., overweight patients with pneumonia treated with ECMO experienced, contrary to previous expectations, a better outcome [20]. It is unsure of how to classify this finding because it is also contradictory to the reasonable argument that obesity may complicate the implantation and maintenance of ECMO. Nevertheless, it must be emphasized that the weight as a predictive factor is assumedly rather questionable because the height and the gender is not considered in the calculation. In another scoring system for ECMO patients, a high BMI is declared as a positive factor for the prognosis [21]. This then again would correspond to the findings of Cho et al.
Another important prognostic factor that appears in both scores is the duration of intubation or mechanical ventilation prior to ECMO. An intubation duration of over 30 hours before ECMO has a score of -4 (SAVE Score), a mechanical ventilation of under 48 hours prior to ECMO amounts to a score of 3 (RESP Score). This suggests that a long intubation and mechanical ventilation time tends to decrease the survival chances. This could be explained by the effects that a long-term intubation has on the critically ill patients. Prolonged intubation and mechanical ventilation may enhance systemic inflammatory processes and increase the risk of ventilator-induced lung injury [22-23]. This allows the assumption that an early implantation of ECMO may be positive for the outcome due to the fact that intubation time before ECMO is reduced. Moreover, a quick and long intubation generally speaks for a critical and potentially life-threatening state that may account for a limited chance of survival.
One of the essential components of the prognosis scores is the diagnosis leading to the implantation of ECMO. The importance of this factor is emphasized by the authors of the scores [6,24]. The diagnoses included in the RESP Score are viral or bacterial pneumonia (score: 3), Asthma (11), Trauma/burn (3), Aspiration pneumonitis (5), other acute respiratory diagnosis (1) and a residual category named non-respiratory and chronic respiratory diagnoses with a score of 0 which, if selected, does not affect the total score. Some diagnoses like Asthma often occur at a younger age. Thus, a correlation with the age can be drawn that it itself is an important prognosis factor. This could yield a relatively good prognosis provided that no severe complications like central nervous system dysfunctions are present. For example, a young patient with trauma-induced ARDS (acute respiratory distress syndrome) has by trend a better outcome than an older sepsis patient with ARDS [25]. In the SAVE Score, the diagnoses myocarditis (score: 3), refractory VT/VF (2) post heart or lung transplantation (3), congenital heart disease (-3) and a residual category named “other diagnoses“ with a score of 0 are available for selection. It can be stated that VT and VF are shockable rhythms that generally have a better prognosis than non-schockable rhythms. However, all the mentioned diagnoses are severe conditions which can be accompanied by serious complications. Why these conditions except congenital heart disease have a positive score is not clearly assessable. In cardiac ECMO, the reversibility of the experienced cardiogenic shock is regarded as being an important predictive factor.
Complications in connection with ECMO occur commonly and are associated with a considerably higher mortality. These can have a big impact on the outcome and therefore play an important role in the scores. Generally, complications can be led back either to the condition of the patient or to the ECMO treatment itself [4]. Complications that affect the central nervous system such as seizures, bleeding and infarction often have devastating effects and can reduce the survival probability drastically. In the RESP Score, this is the item with the most negative score of -7 and also in the SAVE Score it is represented with a score of -3. They frequently lead to irreversible damage and consequently to an early termination of ECMO. Patients with neurologic complications during ECMO have a greater risk for long-term impairment and a significantly higher morbidity and mortality [26]. A further common complication in ECMO patients are infections. In the RESP Score, an associated non-pulmonary infection amounts to a score of -3. The frequency of infections is variable [27]. A distinction must be made between an infection that is related to ECMO and an already preexisting infection as the effect on the prognosis may be quite different [26]. It can be assumed that ECMO patients have a higher susceptibility to infection due to the generally critical condition and the long hospital stays. Furthermore, acute or chronic renal failure is another frequent complication that is associated with a poor outcome [28]. Accordingly, this factor appears in the SAVE Score with a score of -3 or -6, respectively. Studies show that patients with signs of renal failure do not respond well to ECMO [29]. Renal replacement procedures are required in many cases. Liver failure is also considered as a risk factor for an unfavorable prognosis, especially in patients with heart failure or defects [30]. This would fit to the SAVE Score in which liver failure is an item with a score of -3. The alkaline phosphatase and the total bilirubin are presumed to being the key parameters for short- and long-term mortality [30]. Further common complications not incorporated in the scores include bleeding, mechanical issues, cardiopulmonary conditions and metabolic imbalances. Preventing and treating complications adequately may contribute to a better prognosis and could ultimately raise survival chances.
Respiratory parameters such as the PIP (peak inspiratory pressure) and PaCO2 (carbon dioxide partial pressure) are also considered as important predictive factors, especially in patients with respiratory diseases. A high PIP and PaCO2 which indicate a low compliance of the lung is linked to a worse outcome [31]. A low PIP on the other side points to a higher survival chance. In cardiac ECMO, cardiac parameters such as the diastolic blood pressure and pulse pressure before ECMO may also affect the outcome and are therefore part of the SAVE Score. Another risk factor that is included in the scores is the presence of a cardiac arrest prior to ECMO. Due to the seriousness of the condition it stands to reason that this factor decreases survival chances. Yet, the impact on the outcome may presumably be in reality larger than the score of only -2 in the scoring systems suggests. In ECMO patients with respiratory diseases, the administration of certain drugs may also play a role in determining the outcome. Neuromuscular blockade agents are frequently used in ECMO patients to minimize ventilator-induced lung injury and to promote lung recruitment [32]. In the RESP Score, it is considered a protective factor with a score of 1. On the other hand, the application of Bicarbonate infusions or nitric oxide before ECMO have previously been associated with a higher mortality and may therefore worsen the outcome [33-34]. For this reason, they have a score of -2 and -1 in the RESP Score. However, it must be considered that the use of the mentioned drugs is discussed controversially. Many aspects of the application on ECMO patients have yet to be resolved and long-term effects are unknown [34].
CONCLUSION
It can be concluded that the factors which are believed of having a negative impact on the outcome outnumber the protective factors which could be explained by the critical condition of ECMO patients and the relatively high incidence of complications. The prediction of the prognosis through scoring systems is presumably rather difficult due to the complex nature of the issue and the abundance of unpredictable factors. Hence, their accuracy may be considered as questionable. Through the setup of an extensive ECMO database in the clinical facility, a sustainable contribution to optimize procedures can be achieved.
REFERENCES
- Lin CY, Tsai FC, Tian YC, Jenq CC, Chen YC, et al. (2007) Evaluation of outcome scoring systems for patients on extracorporeal membrane oxygenation. Ann Thorac Surg 84: 1256-1262.
- Peigh G, Cavarocchi N, Keith SW, Hirose H (2015) Simple new risk score model for adult cardiac extracorporeal membrane oxygenation: simple cardiac ECMO score. J Surg Res 198: 273-279.
- Lafç G, Budak AB, Yener AÜ, Cicek OF (2014) Use of extracorporeal membrane oxygenation in adults. Heart Lung Circ 23: 10-23.
- Makdisi G, Wang IW (2015) Extra Corporeal Membrane Oxygenation (ECMO) review of a lifesaving technology. J Thorac Dis 7: 166-176.
- Thiagarajan RR, Barbaro RP, Rycus PT, Mcmullan DM, Conrad SA, et al. (2017) Extracorporeal Life Support Organization Registry International Report 2016. ASAIO J 63: 60-67.
- Schmidt M, Bailey M, Sheldrake J, Hodgson C, Aubron C, et al. (2014) Predicting survival after extracorporeal membrane oxygenation for severe acute respiratory failure. The Respiratory Extracorporeal Membrane Oxygenation Survival Prediction (RESP) score. Am J Respir Crit Care Med 189: 1374-1382.
- Pappalardo F, Pieri M, Greco T, Patroniti N, Pesenti A, et al. (2013) Predicting mortality risk in patients undergoing venovenous ECMO for ARDS due to influenza A (H1N1) pneumonia: the ECMO net score. Intensive Care Med 39: 275-281.
- Frenckner B (2015) Extracorporeal membrane oxygenation: a breakthrough for respiratory failure. J Intern Med 278: 586-598.
- Schicker E (2017) Datenbanken und SQL: Eine praxisorientierte Einführung mit Anwendungen in Oracle, SQL Server und MySQL. 5., aktualisierte und erweiterte Auflage. Springer Vieweg, Germany.
- Schubert M (2007) Datenbanken: Theorie, Entwurf und Programmierung relationaler Datenbanken. Vieweg + Teubner Verlag, Germany.
- The Django Book (2020) Django’s Structure – A Heretic’s Eye View - Python Django; 2020.000Z. The Django Book.
- Django (2020) Models | Django documentation | Django.
- Django (2020) The Django template language | Django documentation | Django.
- Ernesti J, Kaiser P (2015) Python 3 : das umfassende Handbuch. Rheinwerk,Germany.
- W3schools (2020) HTTP Methods GET vs POST; W3schools.
- Django (2020) Request and response objects | Django documentation | Django.
- MDN web docs (2020) Über JavaScript. MDN web docs, Mountain View.
- Baek MS, Chung CR, Kim HJ, Cho WH, Cho YJ, et al. (2018) Age is major factor for predicting survival in patients with acute respiratory failure on extracorporeal membrane oxygenation: a Korean multicenter study. J Thorac Dis 10: 1406-1417.
- Horton J. Microsoft Word - ELSO Guidelines General All ECLS Version1.1.doc.
- Cho WH, Oh JY, Yeo HJ, Han J, Kim J, et al. (2018) Obesity survival paradox in pneumonia supported with extracorporeal membrane oxygenation: Analysis of the national registry. J Crit Care 48: 453-457.
- Schmidt M, Zogheib E, Rozé H, Repesse X, Lebreton G, Luyt CE, et al. (2013) The PRESERVE mortality risk score and analysis of long-term outcomes after extracorporeal membrane oxygenation for severe acute respiratory distress syndrome. Intensive Care Med 39: 1704-1713.
- Hemmila MR, Rowe SA, Boules TN, Miskulin J, McGillicuddy JW, et al. (2004) Extracorporeal life support for severe acute respiratory distress syndrome in adults. Ann Surg 240: 595-605.
- Chiu LC, Tsai FC, Hu HC, Chang CH, Hung CY, et al. (2015) Survival predictors in acute respiratory distress syndrome with extracorporeal membrane oxygenation. Ann Thorac Surg 99: 243-250.
- Schmidt M, Burrell A, Roberts L, Bailey M, Sheldrake J, et al. (2015) Predicting survival after ECMO for refractory cardiogenic shock: the survival after veno-arterial-ECMO (SAVE)-score. Eur Heart J 36: 2246-2256.
- Schouten LRA, Bos LDJ, Serpa Neto A, van Vught LA, Wiewel MA, et al. (2019) Increased mortality in elderly patients with acute respiratory distress syndrome is not explained by host response. Intensive Care Med Exp 7: 58.
- Lan C, Tsai PR, Chen YS, Ko WJ (2010) Prognostic factors for adult patients receiving extracorporeal membrane oxygenation as mechanical circulatory support--a 14-year experience at a medical center. Artif Organs 34: 59-64.
- Sun HY, Ko WJ, Tsai PR, Sun CC, Chang YY, et al. (2010) Infections occurring during extracorporeal membrane oxygenation use in adult patients. J Thorac Cardiovasc Surg 140: 1125-1132.
- Antonucci E, Lamanna I, Fagnoul D, Vincent JL, Backer D, et al. (2016) The Impact of Renal Failure and Renal Replacement Therapy on Outcome During Extracorporeal Membrane Oxygenation Therapy. Artif Organs 40: 746-754.
- Chen YC, Tsai FC, Fang JT, Yang CW (2014) Acute kidney injury in adults receiving extracorporeal membrane oxygenation. J Formos Med Assoc 113: 778-785.
- Roth C, Schrutka L, Binder C, Kriechbaumer L, Heinz G, et al. (2016) Liver function predicts survival in patients undergoing extracorporeal membrane oxygenation following cardiovascular surgery. Crit Care 20: 57.
- Rozencwajg S, Pilcher D, Combes A, Schmidt M (2016) Outcomes and survival prediction models for severe adult acute respiratory distress syndrome treated with extracorporeal membrane oxygenation. Crit Care 20: 392.
- Bourenne J, Hraiech S, Roch A, Gainnier M, Papazian L, et al. (2017) Sedation and neuromuscular blocking agents in acute respiratory distress syndrome. Ann Transl Med 5: 291.
- Sabatini S, Kurtzman NA (2009) Bicarbonate therapy in severe metabolic acidosis. J Am Soc Nephrol 20: 692-695.
- Tadphale SD, Rettiganti M, Gossett JM, Beam BW, Padiyath A, et al. (2016) Is Administration of Nitric Oxide During Extracorporeal Membrane Oxygenation Associated With Improved Patient Survival? Pediatr Crit Care Med 17: 1080-1087.
Citation: Regler S, Hulde N, Hoechter D, von Dossow V (2020) Prognosis Scores of Extracorporeal Membrane Oxygenation and Programming of a ECMO Database. J Anesth Clin Care 7: 54.
Copyright: © 2020 Regler S, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.