Bay Cyst Associated with Impacted Third Molar: A Case with an Unusual Radiographic Presentation
*Corresponding Author(s):
Nikhil M KurienDepartment Of Oral And Maxillofacial Surgery, P.M.S College Of Dental Sciences And Research, Kerala University Of Health Sciences, Trivandrum, Kerala, India
Tel:+91 9497273837,
Email:nikhilmkurien@gmail.com
Adersh GA
Department Of Oral And Maxillofacial Surgery, P.M.S College Of Dental Sciences And Research, Kerala University Of Health Sciences, Trivandrum, Kerala, India
Tel:+91 9497273837,
Email:adarsh0004@gmail.com
Vinod Mony
Department Of Oral And Maxillofacial Surgery, P.M.S College Of Dental Sciences And Research, Kerala University Of Health Sciences, Trivandrum, Kerala, India
Tel:+91 9497273837,
Varun MP
Department Of Oral And Maxillofacial Surgery, P.M.S College Of Dental Sciences And Research, Kerala University Of Health Sciences, Trivandrum, Kerala, India
Tel:+91 8891787360,
Email:varunmp@gmail.com
Abstract
Periapical cysts associated with impacted third molars are rare unless they are affected with caries or trauma. Root resorption associated with periapical cysts are common but enamel is resistant to resorption. Here is a case report showing bay cyst associated with an impacted third molar showing an unusual radiographic presentation of crown resorption.
Keywords
INTRODUCTION
Radicular cysts are so far the most common of the cystic lesions that occur in the jaw. It is the sequelae of the most common disease of the tooth, which is dental caries. Besides trauma dental caries is the primary etiological factor of radicular cyst [1]. Radiologically, radicular cysts appear as round or pear shaped unilocular, lucent lesions in the periapical region [2]. They are usually up to 1.5cm in diameter and are bordered by a thin rim of cortical bone [3]. The associated tooth usually has a large carious lesion or an improper restoration. Periapical cysts associated with impacted third molars are very less common unless they are affected with caries. They are formed by degeneration of epithelial rests of malassez as a result of stimulation in the periapical region of the vital or non-vital teeth. It has been revealed microscopically that the pathologic cavity of the radicular cyst is lined by non keratinized stratified squamous epithelium. The fibrous connective tissue wall of the cyst has various degree of infiltration of inflammatory cells and small blood vessels [4,5]. This paper reports the case of a radicular cyst associated with an impacted third molar with an unusual radiographic presentation.
CASE REPORT
A 26 year old male patient reported to the department with the complaint of pain in the lower posterior region of the jaw since two months. The patient had episodes of pain in the same region, which was relieved by analgesics.
Intra oral clinical examination reveals impacted lower left third molar with pericoronal tissue over the distal surface of the tooth (Figure 1). The retromolar tissue was inflamed and tender. The tooth was also tender to percussion. On inspection, occlusal surface had no evidence of dental caries.
 Figure 1: Impacted mandibular third molar showing inflamed pericoronal region.
Figure 1: Impacted mandibular third molar showing inflamed pericoronal region.
Periapical radiograph showed a well-defined ‘S’ shaped radiolucent lesion of approximately 9mm long corono-apically, 3mm long mesio-distally that extends from the coronal aspect of the distal surface of impacted molar extending towards the cement enamel junction, invading the crown distally and then it extends downwards the root (Figure 2). The distal part of the tooth showed loss of radio opaqueness, suggestive of resorption. The distal wall of the pulp chamber and the pulp canal of the distal root also showed resorption. Mesial surface of the crown of the tooth showed radiolucency, suggestive of proximal caries. Panoramic radiograph was made to rule out whether it is an artifact. But the lesion was evident and bone around the lesion also showed resorption (Figure 3). Figure 2: Intra oral periapical radiograph showing ‘S’ shaped lesion.
Figure 2: Intra oral periapical radiograph showing ‘S’ shaped lesion. Figure 3: Panoramic radiograph showing the lesion.
Figure 3: Panoramic radiograph showing the lesion.
Detailed history, clinical and radiographic presentation indicated a differential diagnosis that included entigerous cyst, or a periapical cystor a keratocystic odontogenic tumor. The tooth was surgically removed under local anesthesia and the cavity was curetted. Tooth showed resorption similar to the radiographic appearance (Figure 4). It was interesting to note that the cystic lining was incomplete (Figure 5). The lining was attached to the root of the impacted molar. The histopathological features revealed stratified squamous epithelium that was having 4-5 layers of cell thickness. Fibrous connective tissue wall with spindle-shaped cells are also seen (Figure 6). All these findings pointed towards the diagnosis of radicular cyst. The extraction site exhibited uneventful healing pattern. Figure 4: Surgically removed impacted molar showing resorption.
Figure 4: Surgically removed impacted molar showing resorption. Figure 5: Incomplete lining of the cyst.
Figure 5: Incomplete lining of the cyst.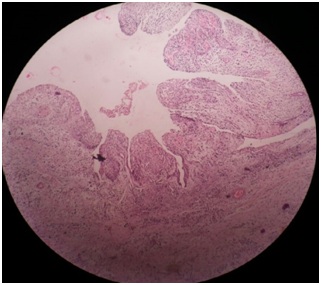 Figure 6: Histopathological findings showing features of periapical cyst.
Figure 6: Histopathological findings showing features of periapical cyst.
DISCUSSION
A radicular cyst is defined as a cyst arising from cell rests of Malassez in the periodontal ligament as consequence of inflammation, usually following the death of dental pulp [1]. Incidence of the periapical cysts varies from 52% [1] to 68% [6] of all jaw cysts. It is higher in third decade of the life [7]. Maxilla is most commonly affected, in which, maxillary anterior teeth are most prone to the cyst. In the mandible, premolars are commonly affected [1,8]. Incidence of cysts occurring in the impacted third molars varies from 0.001% to 3.1%, and dentigerous cysts are the most prevalent types of diagnosed cysts [9]. Incidence of periapical cyst among the periapical pathologies varies from 6% [10] to 55% [11]. Cyst formation is initiated by hydropic degeneration of epithelial cell rests of Malassez as a result of stimulation from non-vital tooth in periapical region [12]. Later many authors have proposed theories behind the development and the progression of the inflammatory periapical cysts which includes osmotic pressure theory that states, the progressive growth of the inflammatory apical cyst is due to the permeability of exudates towards the cystic cavity generated from necrosis of central epithelial cells. This mechanism is applicable to the enlargement of many cysts [13]. Another more specific theory is the abscess theory, which states these lesions can be composed of several components. The differential dynamics of individual components are capable of producing the epithelial proliferation in the abscess area near the apex [14].
Clinically, most of the cases of periapical cysts are asymptomatic. Most of them are usually discovered in the periapical radiographs of symptomatic tooth. They show slow enlargement. Early the enlargement is hard but as the cyst increases in size, the covering bone becomes very thin despite sub periosteal bone deposition and the swelling then exhibits ‘springiness’ or ‘egg shell crackling’. It becomes fluctuant only after entire bone is resorbed. In the maxilla there may be buccal or palatal enlargement. In mandible labial and buccal areas are commonly affected whereas lingual areas show rare involvement. Pain and infection are also seen in some cases (1).In some cases the cyst may be lined with incomplete epithelium just contacting the tooth apex. Such cysts are called as pocket cyst or bay cyst [15].
Unilateral cysts are common [16,17] but bilateral varieties are associated with deciduous teeth [18]. The classic radiological description of radicular cyst is, round or ovoid radiolucent mass covered by a thin radio opaque lining which extends from the lamina dura of the involved tooth [1]. Controversies regarding the size of the cyst are still running. Currently many authors suggest that any lesion below the size of 2cm in diameter cannot be confirmed on radiographs as radicular cyst [1]. Radiological variations are reported in the literature. Bilocular and multilocular varieties of the radicular cysts associated with deciduous teeth are those reported varieties [19].most teeth with periapical cyst are associated with some degree of external root resorption near to the apex of the root [20]. Literatures lack cases of radicular cysts causing crown resorption, which makes our case interesting.
Microscopically the lining is formed by 6 to 20 layers of stratified squamous epithelium. The inflammatory cell infiltrate shows plenty of polymorphonuclear leucocytes whereas the adjacent fibrous capsule is infiltrated by chronic inflammatory cells [1]. Mucous metaplasia and ciliated linings were also reported [16].
CONCLUSION
Our case varies from the normally reported radicular cysts in many aspects. The shape of the cyst was not round or ovoid. It resembles reverse question mark or the shape of the alphabet S. the lining epithelium was not complete. And the crown of the affected tooth showed extensive resorption. Histopathologically the lesion was pocket cyst. But the mystery behind the resorption of the crown remains as such.
REFERENCES
- Shear M, Speight P (2007) Cysts of the Oral and Maxillofacial Regions, (4th edn). Copenhagen: Wiley-Blackwell, New Jersey, USA.
- Goaz PW, White SC (1994) Oral radiology: Principles and interpretation, (3rd edn). Mo: Moshy-Year book, St Louis, Missouri, USA.
- Weber AL (1993) Imaging of cysts and odontogenic tumors of the jaw. Definition and classification. Radiol Clin North Am 31: 101-120.
- Rees JS (1997) Conservative management of a large maxillary cyst. Int Endod J 30: 64-67.
- Tsai CH, Huang FM, Yang LC, Chou MY, Chang YC (2002) Immunohistochemical localization of cyclooxygenase?2 in radicular cysts. Int Endod J 35: 854-858.
- Killey HC, Kay LW, Seward GR (1977) Benign cystic lesions of the jaws: Their diagnosis and treatment, (3rd edn). Churchill Livingston, London, UK.
- Bhaskar SN (1996) Oral surgery-oral pathology conference no. 17, walter reed army medical center: Periapical lesions-types, incidence, and clinical features. Oral Surgery, Oral Medicine, Oral Pathology 21: 657-671.
- Borg G, Persson G, Thilander H (1974) A study of odontogenic cysts with special reference to comparisons between keratinizing and nonkeratinizing cysts. Sven Tandlak Tidskr 67: 311-325.
- Güven O, Keskin A, Akal ÜK (2000) The incidence of cysts and tumors around impacted third molars. Int J Oral Maxillofac Surg 29: 131-135.
- Sommer RF (1966) Clinical endodontics (3rd edn). W.b. Saunders Co, Philadelphia, USA.
- Priebe WA, Lazansky JP, Wuehrmann AH (1954) The value of the roentgenographic film in the differential diagnosis of periapical lesions. Oral Surg Oral Med Oral Pathol 7: 979-983.
- Keinan D, Cohen RE (2013) The significance of epithelial rests of malassez in the periodontal ligament. J Endod 39: 582-587.
- Nair PN (1997) Apical periodontitis: A dynamic encounter between root canal infection and host response. Periodontol 2000 13: 121-148.
- Nair PN, Sundqvist G, Sjögren U (2008) Experimental evidence supports the abscess theory of development of radicular cysts. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 106: 294-303.
- Nair PN (1998) New perspectives on radicular cysts: Do they heal? Int Endod J 31: 155-160.
- Joshi NS, Sujan SG, Rachappa MM (2011) An unusual case report of bilateral mandibular radicular cysts. Contemp Clin Dent 2: 59-62.
- Holla VA, Chatra L, Shenai P, Rao PK, Veena KM, et al. (2012) Bilateral inflammatory cysts of the jaw: Report of an unusual case. Imaging Sci Dent 42: 105-109.
- Gaynor WN (2012) Bilateral radicular cysts of mandibular deciduous teeth: A case report. N Z Dent J 108: 106-109.
- Lustmann J, Shear M (1985) Radicular cysts arising from deciduous teeth: Review of the literature and report of 23 cases. Int J Oral Surg 14: 153-161.
- Malueg LA, Wilcox LR, Johnson W (1996) Examination of external apical root resorption with scanning electron microscopy. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 82: 89-93.
Citation: Kumar S, Kurien NM, Adersh GA, Mony V, Varun MP (2019) Bay Cyst Associated with Impacted Third Molar: A Case with an Unusual Radiographic Presentation. J Dent Oral Health Cosmesis 4: 011.
Copyright: © 2019 Surej Kumar, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.