Hemangioma of the Jejunum as the Cause of Anemia in the Child
*Corresponding Author(s):
Gorelik ADepartment Of Polytrauma, Clinical And Research Institute Of Emergency Pediatric Surgery And Trauma (CRIEPST), Moscow, Russian Federation
Tel:+7 4956335828,
Email:dr.a.gorelik@gmail.com
Abstract
Hemangioma of Digestive Tract (DT) is a benign vascular neoplasm with localization at various parts of the intestinal tube. Clinical significance of gastrointestinal tract hemangiomas usually associates with such complications as gastro-intestinal bleedings, intussusceptions, intestinal obstruction or intestinal perforation.
Purpose: A case-report of a rare clinical observation of a jejunal cavernous hemangioma causing recurrent intestinal bleedings.
Patients and methods: An 11-year-old boy was presented at our hospital with a chronic anemia and recurrent intestinal bleedings of unclear etiology. A comprehensive diagnostic examination was performed including both laboratory and instrumental techniques, such as digestive tract examination with video-capsular technique and angiography of the abdominal cavity.
Results: Video-capsular examination revealed a vascular neoplasm in jejunum which was suspected to be a possible source of bleeding. Further angiography examination has confirmed the vascular structure of the neoplasm. Laparoscopy revealed a cavernous hemangioma, about 1.5 cm in diameter, located in the jejunum wall and proliferating into intestinal lumen both from intestinal wall and serous membrane. Part of the jejunum was respected using microlaparotomic approach in the umbilical area with end-to-end anastomosis. The diagnosis was confirmed morphologically. The post-operative period was uneventful.
Conclusion: Cavernous hemangiomas of jejunum are extremely rare and difficult to be diagnosed as a cause of recurrent intestinal bleedings. The timely employment of modern diagnostics and surgical techniques results in a mini-invasive treatment approach that leads to a cost-effective care and rapid patient's recovery.
Keywords
INTRODUCTION
Hemangioma of Digestive Tract (DT) is a benign vascular neoplasm. There are two main histological types of hemangiomas: capillary and cavernous, they can also be of mixed type [1-3]. Hemangiomas can have degenerative changes, such as calcination, thromboses and hyalinization.
Capillary hemangiomas are neoplasms consisting of branching vessels of capillary type with a narrow lumen which is not always filled with blood. Macroscopically, formations are red or cyanotic nodes with smooth or tuberous surface.
Cavernous hemangiomas, that consist neoplasms that consist of blood-filled spaces or sinuses covered with a single-layer or multilayer endothelium. Macroscopically they look like scarlet-cyanotic nodes separated from the surrounding tissues and resembling a sponge on the cut. Most often they look like intraluminal polypoid formations or infiltrative submucosal and intramural masses which may protrude into mesentery.
While hemangiomas can be located at any part of the intestinal tract, they usually occur in the small intestine and can be solitary or describe the syndromes in which multiple hemangiomas occur. Often similar lesions can be found in other organs such as liver or skin. Most DT hemangiomas are located in the small intestine. Hemangiomas of the small intestine account for no more than 5% of all neoplasms in DT [4,5]. These lesions occur 1.5 times more often in men than in women. Most often the neoplasms are found in the jejunum. This disease is extremely rare in children [3-6]. A small number of similar clinical observations has been reported in literature [3-7].
Most often small intestine hemangiomas manifest clinically as intestinal hemorrhage, less often as intestinal obstruction, perforation or intussusception [6,7].
Gastrointestinal bleedings can be either massive and life-threatening or nonintensive and undetectable, this erodes clinical picture and makes the diagnostics process difficult, time-consuming and ineffective.
We present a rare case observation of jejunal cavernous hemangioma in a child that caused a recurrent intestinal bleeding, the main clinical manifestation of which was a chronic Iron Deficiency Anemia (IDA).
An 11-year-old boy was complaining of a chronic anemia and suspected recurrent intestinal bleeding of unclear etiology. According to his mother the child has been repeatedly examined at various medical institutions for iron deficiency anemia. He had a dark-colored stool from time to time in the past six months; there were no clinical manifestations of gastrointestinal bleeding before that.
Child’s early development was age appropriate. At the age of 1 he had a surgical removal of intermuscular cyst on the anterior abdominal wall (histological findings-hemangioma); at the age of 3- a hemangioma on the heel was excised.
DISEASE HISTORY
The boy complained of an increased fatigue for the first time at the age of 8, his mother has noticed pale skin. The child was examined at a local out-patient unit and was diagnosed with moderate anemia on the basis of blood test results.
Hospital examination: Ultrasound of the abdominal cavity, esogastroduodenscopy (EGDS), colonoscopy and MRI of the abdominal cavity. No pathology was identified.
The child was under hematologist’s observation with an iron-deficiency anemia diagnosis and was prescribed iron products. At the age of 9 patient’s hemoglobin level dropped down again to 85 g/l. Anemia was worsening despite of restarted iron products intake and hemoglobin levels were still low about 70 g/l. The child was repeatedly examined in a hospital: no evidence of gastrointestinal bleeding was found; oncohematological pathology was ruled out based on bone marrow examination. CT of the abdominal cavity revealed volumetric (neoplastic) formations in the abdominal cavity. The child was discharged home following severe anemia correction. 4 months later he was hospitalized again with persisting iron deficiency anemia. He underwent the traditional laboratory-instrumental examination (EGDS, colonoscopy and MRI of the abdominal cavity) to exclude gastrointestinal hemorrhage and indentify a possible source of anemia. Once again there were no findings indicative of bleeding. Anemia was suppressed by a repeated course of iron products. However two months later hemoglobin levels dropped again down to 78 g/l. The child was hospitalized and examined by a gastroenterologist who excluded Inflammatory Bowel Diseases (IBD) as a possible cause of anemia: EGDS, colonoscopy and ultrasound of the abdominal cavity, MRI of the abdomen. Once again there was no data indicating gastrointestinal bleeding or IBD.
Following hospital discharge the child, then 10, underwent genetic examination recommended by his hematologist: IRIDA - iron-resistant IDA (2 heterozygous mutations) was identified.
Iron products were recommended parenterally, which resulted in several hospital admissions to pediatric departments. The anemia remission did not correspond to administered iron dosage however, within 2-3 weeks hemoglobin levels dropped again. It was then for the first time that the child had an episode of a tarry stool which was accompanied by hemoglobin decrease down to 42 g/l; he was hospitalized again for the erythrocyte mass transfusion. The child was admitted to the Clinical and Research Institute of Emergency Pediatric Surgery and Trauma (CRIEPST) to have a video-capsular DT examination when he was 11 years old. On admission his hemoglobin was at 84 g/l. The images of distal parts of the jejunum revealed a volumetric vascular formation of a blue-purple color, round in shape, 1.5 cm in diameter, partially covered with fibrin and proliferating into the lumen of the intestine. Hemangioma of the jejunum was suspected (Figure 1). Three-phase contrasting CT angiography did not reveal any findings to correlate for this mass. Conventional angiogram of the abdominal vessels however, demonstrated a focal contrast collection on delayed venous phase overlying small bowel loops, suggestive of a hypervascular lesion possibly arising from the small intestinal wall (Figure 2).

Figure 1: Cavernous hemangioma of the jejunum - Video capsular examination.
 Figure 2: A hypervascular formation in the small intestine - Angiography of abdominal vessels.
Figure 2: A hypervascular formation in the small intestine - Angiography of abdominal vessels.
Collectively, these findings are concerning for a vascular lesion in the distal small intestine causing recurrent GI hemorrhage and ultimately chronic IDA. The surgical plan included laparoscopic revision of the small intestine with enteroscopy, if necessary, to evaluate a formation and to decide on surgical tactics intraoperatively. During laparoscopy of distal parts of the ileum an intraluminal formation of cyanotic color was found, which was 1.5 cm in diameter, invading the intestinal wall and visible through the serous membrane of the intestine (Figures 3a & 3b). The incision along the lower circumference of the umbilicus was enlarged to 3 cm for the optical trocar. The ileum loop with the lesion was instrumentally fixed and took out through the wound. Enterotomy was performed. An intraluminal formation of a spongy structure was identified at audit, which was a dark purple color, round-shaped, about 1.5 cm in diameter, invading into the intestinal wall to the serous membrane (Figure 4). The macroscopic picture of the formation corresponded to that of a cavernous hemangioma. Part of the ileum with the formation was resected with end-to-end single suture anastomosis, vikril 4/0 (Figure 5).

Figure 3: Cavernous hemangioma in the jejunum with intralumenal location (a) and with invasion into the intestinal wall till the serous layer (b) Laparoscopy.
 Figure 4: Cavernous hemangioma of the jejunum-Minilaparotomy, enterotomy.
Figure 4: Cavernous hemangioma of the jejunum-Minilaparotomy, enterotomy.

Figure 5: "End-to-end" anastomosis-Minilaparotomy.
The diagnosis of cavernous hemangioma was confirmed by histological findings: numerous, predominantly of venous type, vessels and cavities lined with endothelial cells were identified in the submucosa and in the muscle layer of the small intestine (Figure 6).
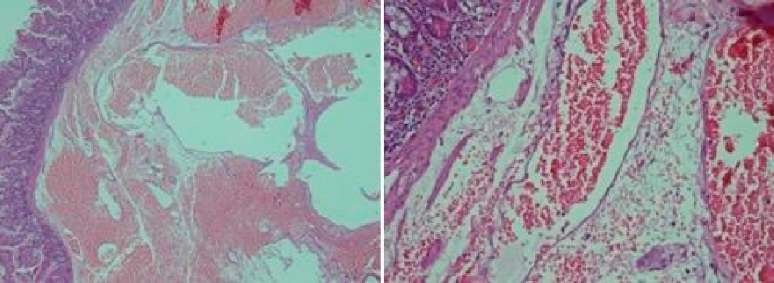
Figure 6: Micropreparation.
The postoperative period was uneventful. There were no DT passage disorders or systemic inflammatory reactions. Since day 1 the child had an enteral load: spilled food and sip feeding. The patient had an independent stool on day 2. On day 7 following the surgery hemoglobin level were at 108 g/l and the patient was subsequently discharged to home. Results of catamnestic examinations at 2 and 4 months: no complaints, hemoglobin at 117 and 132 g/l, respectively.
DISCUSSION
The clinical case above shows an extremely rare pathology in children, hemangioma of the jejunum, which was a source of recurrent intestinal bleedings. Despite repeated in-patient examinations with modern expensive procedures, the cause of anemia remained unidentified and the patient received just symptomatic not etiologic treatment. It should be noted that modern diagnostics allows examining the entire intestinal tube for possible sources of bleeding and should be a mandatory procedure in anemia patient’s examination [8-10]. Video-capsular examination is suitable for this task and should be considered part of initial diagnostic process during intraluminal endoscopy together with EGDS and colonoscopy. This approach would assist in establishing a diagnosis more efficiently, leading to appropriate patient treatment and would allow to cure a patient quicker with associated economic benefits. Angiography allows confirming diagnosis and specifies vascular genesis in neoplasms which is important for further surgical treatment planning. In this clinical case we observed that the removal of two soft tissue hemangiomas at a very early age in patient’s anamnesis was left without attention. These procedures should have made one suspect DT hemangioma as a possible cause of bleeding and anemia. Therefore the usage of entire arsenal of in-patient diagnostic capabilities in a timely manner allows the most accurate diagnosis verification and helps to develop most rational surgical tactics in order to minimize surgical aggression. The front abdominal wall after the surgery in (Figure 7).

Figure 7: The front abdominal wall after the surgery.
CONCLUSION
Iron deficiency anemia may be caused by small intestine hemangioma’s hemorrhage that does not have any clinical manifestations of the intestinal bleeding. Examination protocol for patients with iron deficiency anemia should include examination procedures for all sections of the intestinal tube, including video-capsular DT examination.
REFERENCES
- Boyle L, Lack EE (1993) Solitary cavernous hemangioma of small intestine. Case report and literature review. Arch Pathol Lab Med 117: 939-41.
- Shi CS, Li G, Wang YL (2011) Clinical characteristics and diagnosis of small intestine hemangioma in children. Zhonghua Er Ke Za Zhi 49: 474-476.
- Magnano A, Privitera A, Calogero G, Nanfito L, Basile G, et al. (2005) Solitary hemangioma of the small intestine: an unusual cause of bleeding diagnosed at capsule endoscopy. J Pediatr Surg 40: 25-27.
- Huber A, Abdel Samie A, Kychenko D, Theilmann L (2012) A rare cause of recurrent iron-deficiency anemia: cavernous hemangioma of the small intestine. J Gastrointestin Liver Dis 21: 343.
- Bae SJ, Hwang G, Kang HS, Song Hj, Chang WY, et al. (2015) Single Cavernous Hemangioma of the Small Bowel Diagnosed by Using Capsule Endoscopy in a Child with Chronic Iron-Deficiency Anemia. Clin Endosc 48: 340-344.
- Sakaguchi M1, Sue K, Etoh G, Takagishi T, Ezaki T et al. (1998) A Case of Solitary Cavernous Hemangioma of the Small Intestine with Recurrent Clinical Anemic Attacks in Childhood. J Pediatr Gastroenterol Nutr 27: 342-343.
- Park J (2012) Large Cavernous Hemangioma in the Jejunum of a 2-year-old Boy Treated by Laparoscopy-assisted Resection. J Korean Assoc Pediatr Surg 18: 24-29.
- Liu W, Xu C, Zhong J (2009) The diagnostic value of double-balloon enteroscopy in children with small bowel disease: report of 31 cases. Can J Gastroenterol 23: 635-638.
- Oikawa-Kawamoto M, Sogo T, Yamaguchi T, Tsunoda T, Kondo T, et al. (2013) Safety and utility of capsule endoscopy for infants and young children. World J Gastroenterol 19: 8342-8348.
- Bar-Meir S, Eliakim R, Nadler M, Barkay O, Fireman Z, et al. (2004) Second capsule endoscopy for patients with severe iron deficiency anemia. Gastrointest Endosc 60: 711-713.
Citation: Karaseva OV, Gorelik AL, Kharitonova AYu, Kislykov AN, Filinov IV (2018) Hemangioma of the Jejunum as the Cause of Anemia in the Child. J Emerg Med Trauma Surg Care 5: 022.
Copyright: © 2018 Karaseva OV, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.