QSOFA and Body Temperature: A Simple Strategy for Evaluate Cirrhotic Patients with Sepsis in Emergency Unit?
*Corresponding Author(s):
DiMicoli ADepartment Of Emergency Medicine, Sant’Orsola-Malpighi University Hospital, Via Massarenti 9, 40138 Bologna, Italy
Tel:+393403369979,
Email:antonio.dimicoli@aosp.bo.it, antoniodimicoli@gmail.com
Abstract
Cirrhotic patients have a high risk of developing sepsis: an early diagnosis is essential for their management. The quick Sequential Organ Failure Assessment (qSOFA) is an accepted tool to identify patients with suspected infection at risk of negative evolution.This study aims to evaluate whether qSOFA can predict the risk of intra-hospital mortality in cirrhotic patients with suspected infection presenting in the Emergency Department; moreover this study aims to evaluated if a new score, T-qSOFA (that altered if qSOFA was ≥ 2 or body temperature >38°C), increases the accuracy of qSOFA.
Methods
qSOFA and T-qSOFA were calculated in 108 cirrhotic patients with suspected infection enrolled during 24 months.
Results
qSOFA was ≥ 2 in 9 patients whereas T-qSOFA was altered in 27.20 patients died (4 with qSOFA ≥2 and 7 with temperature >38°C). qSOFA had a high specificity to identifying patients with better prognosis but its sensitivity is low. “T-qSOFA” increases sensitivity a2nd positive predictive value and became an independent predictor of mortality in the multivariate analysis.
Conclusion
qSOFA has good prognostic accuracy in patients with cirrhosis and suspected infection; T-qSOFA is an excellent, reproducible and quickly obtainable instrument to discriminate the risk of adverse prognosis in cirrhosis.
Keywords
INTRODUCTION
Following the new proposed criteria, sepsis is defined as a life-threatening organ dysfunction caused by a deregulated host response to infection. Thus, the role of systemic inflammation to organ dysfunction is central, and it is now defined as an acute change in Sequential Organ Failure Assessment (SOFA) score ≥ 2 points from baseline (Sepsis-3) [4].
The SOFA score is based on the following specific parameters: mean arterial blood pressure, platelet count, bilirubin blood levels, Glasgow Coma Scale (GCS), blood creatinine levels, ratio of oxygen partial pressure in arterial blood and inspirited fraction of oxygen. Septic shock is identified in patients in whom sepsis is associated with necessity of use of vasopressors to maintain Mean Arterial Pressure (MAP) ≥ 65 mmHg (circulatory failure) and levels of serum lactate ≥ 2 mmol/l (alteration of cellular metabolism). Considering the difficulty of calculating SOFA score outside the Intensive Care Unit (ICU), a simplified tool has been proposed to quickly identify patients with suspected infection at risk of negative evolution (death or prolonged hospitalization in ICU): the Quick SOFA (qSOFA). This score is calculated exclusively on parameters easily deductible in an emergency context: respiratory rate > 2/min, altered state of consciousness and sistolic blood pressure < 100 mmHg. It is positive if at least two of these parameters are altered. qSOFA is validated to quickly recognize potentially infected patients with a worse prognosis and a high risk of mortality [5].
These scores (SOFA and qSOFA) however have never been validated on cirrhotic patients with suspected infection presenting in the Emergency Department (ED). Firstly, this study aims to evaluate whether qSOFA can predict the risk of intra-hospital mortality in this population. Secondly, is evaluated if a new simply score, T-qSOFA that include body temperature > 38°C, increases the accuracy of qSOFA.
MATERIAL AND METHODS
If the same patient has made more visits in ED in the enrolment period, all visits were considered individually. Demographic, clinical, haemodynamic,neurological, hemogasanalytic, laboratory and ultrasound data (presence of ascites) were collected for each patient at ED. Based on these data, qSOFA, SOFA, Model for End-Stage Liver Disease (MELD) [7] and Child-Pugh [8] scores were calculated.
A new simply and dichotomous variable, named T-qSOFA, has been created: if body temperature is≥ 38°C or qSOFA ≥ 2 its value is 1, in other case its value is 0.Patients were followed until discharge or eventual death; the duration of hospitalization was also recorded and the site of infection reported, if identified. The protocol was approved by the local ethics committee of the Hospital, and all patients provided written informed consent.
The statistical variables were expressed as mean ± standard error or median and range, in the most appropriate way based on their distribution. The Pearson and Spearman tests were used to evaluate correlations between the analysed variables and mortality. A value of p <0.05 was considered statistically significant. Univariate and multivariate Cox regression analyses of predictors of mortality were performed using a competiting risk approach with Fine and Gray method, and the result expressed as p value. Variables found to be associated with in-hospital mortality with a p value <0.1 in the univariate analysis were included in a multivariate analysis with stepwise backward elimination (entry p < 0.05, drop p > 0.1). The statistical analysis was performed using SPSS v 22.0 statistical package.
RESULTS
|
Demographic Data |
|
|
Male |
54 patients |
|
Female |
54 patients |
|
Age |
67 ± 0.8 years |
|
Laboratoristic Data |
|
|
Total bilirubin (mg/dL) |
3.6 ± 0.4 |
|
C Reactive- protein (mg/dL) |
5.2 ± 0.6 |
|
Creatinine (mg/dL) |
1.4 ± 0.7 |
|
INR |
1.7 ± 0.9 |
|
Platelets (x 103/mmc) |
115.2 ± 8.1 |
|
Leukocytes (x 103/mmc) |
8.7 ± 6.5 |
|
Albumin (g/L) |
3.1 ± 0.1 |
| Hemodynamic Data | |
|
Systolic blood pressure (mmHg) |
122.2 ± 10.1 |
|
Diastolic blood pressure (mmHg) |
70.4 ± 8.3 |
|
Heart rate (bpm) |
85.2 ± 7.3 |
|
Breath frequency (acts per minutes) |
14.0±2.1 |
|
Partial saturation of oxygen (%) |
96.2 ±3.2 |
|
Ascitic decompensation |
55 patients (50%) |
| Clinical Data | |
|
Altered state of consciousness |
20 patients (18%) |
|
Fever |
49 patients (45%) |
| Main Scores | |
|
MELD |
16.2 ± 0.8 |
|
Child - PughScore (A:B:C) |
22:53:33 |
|
Infection Site |
Cases |
% |
|
Respiratory system |
22 |
20 |
|
Urinary system |
22 |
20 |
|
Skin |
10 |
9 |
|
Cholangitis |
6 |
6 |
|
Cholecystitis |
6 |
6 |
|
Spontaneous bacterial peritonitis |
6 |
6 |
|
Pancreatitis |
4 |
4 |
|
Colitis from C. difficile |
2 |
2 |
|
Gastroenteritis |
2 |
2 |
|
Pericholecystic abscess |
2 |
2 |
|
Acute appendicitis |
1 |
1 |
|
Peritonitis |
1 |
1 |
|
Rectal KPC |
1 |
1 |
|
Media otitis |
1 |
1 |
|
Visceral Leishmania |
1 |
1 |
|
Endocarditis |
1 |
1 |
|
Undefined site |
24 |
22 |
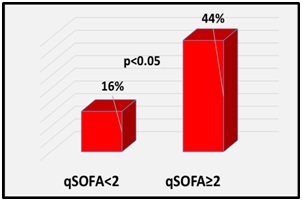
During hospitalization 20 patients died (18.5%), of whom 4 with qSOFA ≥ 2 and 7 with temperature > 38°C. In the subgroup of patients with qSOFA ≥ 2, mortality was 44.4%, while among patients with qSOFA < 2 it was 16.1% (p< 0.05)(Figure 2). In the subgroup of patients with temperature >38°C mortality was 40.7 %. The death occurred on 17th±2 days of hospitalization for patients with a qSOFA ≥ 2 and on 23rd± 3 days for others. This time does not statistically significantly differ between the two subgroups.
Sensitivity, specificity, positive and negative predictive value of qSOFA and T-qSOFA to predict mortality has benne calculated as indicated in table 3. In univariate analysis MELD, qSOFA, sistolic blood pressure, body temperature, T-qSOFA, transfer to ICU, PCR, creatinine, INR, arterial blood, pH are statistically significant prognostic factors of mortality. Instead, considering the subgroup of patients with qSOFA<2, MELD and the variables that determine it, PCR and body temperature have been predictors of mortality in univariate analysis. Only T-qSOFA is predictors of mortality in multivariate analysis.Only 5 patients were transferred to ICU after evaluation in ED, including 4 with qSOFA ≥ 2 (p <0.00001) and all 5 with SOFA ≥ 2 and T-qSOFA = 1.
|
|
Sensitivity |
Specificity |
Positive |
Negative Predictive Value |
|
Predictive Value |
||||
|
qSOFA |
20.00% |
94.30% |
44.40% |
83.40% |
|
T-qSOFA |
55.00% |
81.8.0 % |
40.70% |
88.90% |
|
p value |
0.01 |
ns |
ns |
0.01 |
DISCUSSION
In other setting, SOFA score proved to fit to identify quickly septic patients in an emergency unit [9]. However, SOFA score requires the availability of a previous evaluation to the development of bacterial infection, in order to be able to calculate the deterioration. This represents a limit to the application of SOFA score in cirrhotic patients, who often have pre-existing conditions of organ failure: therefore it is necessary to have an instrument that does not depend on the previous clinical conditions and on the results of laboratory tests.
Unlike SOFA score, qSOFA does not require any previous evaluation. Moreover, in the context of ED, an easy instrument used at bed-side, such as qSOFA, is necessary. This is the first study that evaluate, in a third level Hospital, the accuracy of this score in these group of patients. During the follow up we described a mortality (18%) comparable with other studies [10]. In our results, qSOFA shows high specificity to identifying patients with better prognosis, which only require conservative management approach. Instead, sensitivity of qSOFA is poor in identifying patients who later die and is only a predictor of mortality in univariate analysis. The low sensitivity of qSOFA to predict mortality in this study may be due to both factors; first, the limited number of patients included in the study; second, at the time of access to the ED the parameters of qSOFA could not be altered because most of these patients suddenly arrived at ED so strictly and frequently evaluated by the hepatologist physician: as soon as the first non-specific symptoms of the infection appear, they suggested to get to ED.
A qSOFA ≥ 2 has the role of directing physicians to perform further diagnostic tests for organ dysfunction, to start or enhance an adequate therapy and possibly decide to enhance patient’s monitoring up to transfer to ICU. The addition of body temperature >38°C (objective and easily determinable parameter in an emergency context) to score in a new score “T-qSOFA” not only statistically increases both sensitivity (35%) and positive predictive value (58%) but also became an independent predictor of mortality to the multivariate analysis. Moreover, this new variable does not significantly decrease specificity and positive predictive value.
A simple and available action as the measurement of body temperature could significantly improve the management of cirrhotic patients with sepsis in the ED.This paper presents some limits. First, the study wad lead in a single centre that is a third level hospital for cirrhotic patients: so a selection bias is unavoidable; however, in our Hospital are often evaluated cirrhotic patients with a high MELD that most frequently develop sepsis. Second, the sample size is low so the results can be mainly influenced overall about the ICU access.Third the retrospective method does not permit any hope to deduce some data.
In conclusion, this study shows that, in a population of patients with liver cirrhosis and suspected infection presenting to ED of a third level centre, qSOFA has good specificity and good negative predictive value; in addition it is easily applicable, reproducible and it is quickly obtainable due to no need of diagnostic tests waiting that can slow down therapeutic decisions. Therefore, in addition to clinical judgment, a new score named qt-SOFA is an excellent instrument to discriminate the risk of adverse prognosis in cirrhotic patients.
Surely the failure to achieve two or more criteria of qSOFA should not delay the treatment of the infection in the cirrhotic patient. In this sense, both qSOFA and T-qSOFA cannot be considered a screening test for sepsis.Other prospective and multicentre study are necessary in the future to evaluate better the validity of this scores.
REFERENCES
- Gustot T, Durand F, Lebrec D, Vincent JL, Moreau R (2009) Severe sepsis in cirrhosis. Hepatology 50: 2022-2033.
- Jalan R, Fernandez J, Wiest R, Schnabl B, Moreau R, et al. (2014) Bacterial infections in cirrhosis: A position statement based on the EASL Special Conference 2013. J Hepatol 60: 1310-1324.
- Fernàndez J, Gustot T (2012) Management of bacterial infections in cirrhosis. J Hepatol 56 1: 1-12.
- Singer M, Deutschman CS, Seymour CW, Shankar-Hari M, Annane D, et al. (2016) The third international consensus definitions for sepsis and septic shock (Sepsis-3).JAMA 315: 801-810.
- Freund Y, Lemachatti N, Krastinova E, Van Laer M, Claessens YE, et al. (2017) Prognostic accuracy of sepsis-3 criteria for in-hospital mortality among patients with suspected infection presenting to the emergency department. JAMA 317: 301-308.
- Mazzaferro V, Regalia E, Doci R, Andreola S, Pulvirenti A, et al. (1996) Liver transplantation for the treatment of small hepatocellular carcinomas in patients with cirrhosis. N Engl J Med 334: 693-699.
- Kamath PS, Kim WR (2007) The model for end-stage liver disease (MELD). Hepatology 45: 797-805.
- Pugh RN, Murray-Lyon IM, Dawson JL Pietroni MC, Williams R (1973) Transection of the oesophagus for bleeding oesophageal varices. Br J Surg 60: 646-649.
- Raith EP, Udy AA, Bailey M, McGloughlin S, MacIsaac C, et al. (2017) Prognostic accuracy of the SOFA score, SIRS criteria, and qSOFA score for In-Hospital mortality among adults with suspected infection admitted to the intensive care unit. JAMA 317: 290-300.
- Arvaniti V, D’Amico G, Fede G, Manousou P, Tsochatzis E, et al. (2010) Infections in patients with cirrhosis increase mortality four-fold and should be used in determining prognosis. Gastroenterology 139:1246-1256 .
Citation: DiMicoli DA, Nizza D, Cavazza M (2019) qSOFA and Body Temperature: A Simple Strategy for Evaluate Cirrhotic Patients with Sepsis in Emergency Unit. J Emerg Med Trauma Surg Care 6: 029.
Copyright: © 2019 DiMicoli A, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.