Surgical Management of Gingival Recession Using free Gingival Autograft: Case Series
*Corresponding Author(s):
Rajkumar MeenaDepartment Of Periodontics, Rajasthan University Of Health Sciences -College Of Dental Sciences, Rajasthan, India
Tel:+91 7891791938,
Email:rajkumarmeena561@gmail.com
Abstract
The aim of this clinical case series is to describe surgical management of Miller’s Class II recession in lower anterior using Free Gingival autograft. The free gingival graft is an effective treatment in increasing the width of mandibular keratinized tissue and maintain an inflammation free state.
Introduction
Gingival recession is characterized by apical migration of marginal gingiva, which may lead to compromised esthetics, root sensitivity, root caries, and/or pulp hyperemia. Several techniques are there for of management of gingival recession, those are, Free Gingival Grafts [FGGs], subepithelial connective tissue graft, pedicled grafts, lateral and coronal, etc.,[1] FGGs were initially described by Bjorn, in 1963 [2]. The term FGG was coined by Nabers [3]. Since then, they have been used to cover denuded root surfaces, to increase the width and thickness of attached gingiva. The benefits of FGG are its high predictability and relative ease of technique.
Case Report
Case 1
A 31-year-old female patient reported to the Department of Periodontology, RUHS- College of Dental Sciences, Jaipur with a chief complaint of progressive downward shifting of gum in lower front teeth region along with tooth sensitivity. There was no obvious medical history. Clinical examination revealed moderate plaque accumulation, simplified Oral hygiene index score was 1.9 . Gingival Recession was Miller’s class II with respect to 41. The gingival biotype was thin. The width of attached gingiva was 1mm and had coronal frenum attachment. The recession noted was ‘U’ type recession with 4 mm apicocoronal height and 3 mm mesio-distal width (Figure 1).
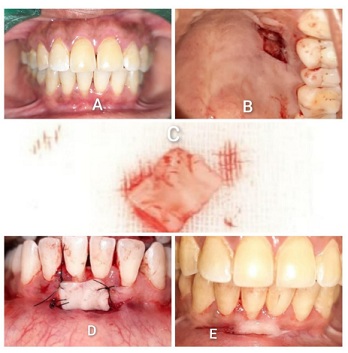 Figure 1: Free gingival autograft in 41.
Figure 1: Free gingival autograft in 41.
Case 2
A 32 years female reported to the Department of Periodontology, RUHS- College of Dental Sciences, Jaipur with a similar chief complaint. There was no obvious medical history. Clinical examination revealed moderate plaque accumulation, simplified Oral hygiene index score was 2.2. Gingival Recession was Miller’s class II with respect to 31. The gingival biotype was thin and had coronal frenum attachment. The recession noted was ‘U’ type recession with 3 mm apicocoronal height and 3 mm mesio-distal width (Figure 2).
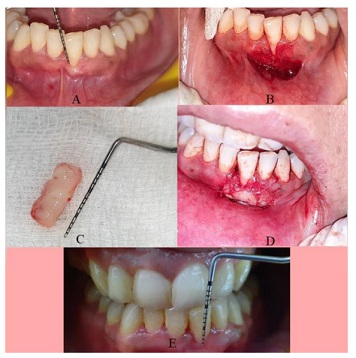 Figure 2: Free gingival Autograft in 31.
Figure 2: Free gingival Autograft in 31.
Procedure
Preparation of recipient site
The purpose of this step was to prepare a firm connective tissue bed to receive the graft. After local anesthesia with 2% lignocaine and intraoral disinfection was done with 0.2 % chlorhexidine mouthrinse. The recessed tooth was planed thoroughly with a Gracey 1-2 curette in both the cases. The site was prepared by with # 15 blade. Horizontal incisions were made in the two interdental papillae adjacent to the recession area to be covered. These incisions were made at the level of the cementoenamel junction and were extended to the line angles of the adjacent teeth. The horizontal incisions were made at a 90degree angle to the gingival surface, creating a well-defined butt joint margin. Two oblique vertical incisions were then placed at the distal ends of the horizontal incisions and were extended beyond the mucogingival line. Periosteum was left covering the bone. A partial thickness flap was elevated and excised apically and a recipient bed measuring 12 mm × 7 mm was prepared. Root biomodification was done by tetracycline hydrochloride 50 mg/ml for 3 minutes.
Preparation of donor sit
The graft consist of epithelium and a thin layer of underlying connective tissue. The graft was planned to be retrieved from distal to anterior palatine rugae area with respect to tooth number 24, 25, and 26. Greater palatine nerve block was given using same anaesthetic solution as used for the recipient site. Tin foil template of 15×7 mm was placed on the donor site and bleeding points were induced. # 15 blade was inserted to desired thickness at one edge of the graft. The graft was elevated from one edge and was held with tissue forceps. The graft was separated with the blade by lifting it gently. Thus, a graft was obtained from the palate. The underside of graft was checked for any fatty or glandular tissues. The tissue tags and fatty tissues were removed and graft of uniform thickness of about 1.5 mm thickness was prepared using #15 scalpel.
Transfer and immobilize the graft
Excess clot was removed from the recipient site. The graft was positioned and adapted firmly to the recipient site. The graft was secured in the recipient site with interrupted sutures. The graft was completely immobilized.
Discussion
Gingival recession defects create unfavourable contour of the gingival margin and creates an esthetic defect [4].Various mucogingival surgeries have been described for the treatment of gingival recession to maintain an inflammation free area and retain a stable level of attachment for prolongedperiods of time [5]. FGG accomplish three objectives those are enhances plaque removal around gingiva, improves esthetic and ensure an adequate epithelial seal [6].
There are two basic surgical techniques for the free gingival graft for root coverage. The technique proposed by Miller [7]. is a one-step procedure or the direct approach whereas the other one described by Bernimoulin et al., [8] involves two surgical steps and is referred to as the indirect approach. Both the above cases were performed by direct approach.
The survival of the graft depends on the re-storing of an adequate blood supply in its new position. Anything that disturbs the nourishment of the grafted tissue will have a negative impact on its survival. Healing is divided into three phases initial (plasmic circulation) phase, (re)vascularization phase and tissue maturation (organic union) phase [9].
Primary root coverage, occurs immediately following grafting, is due to bridging that is persistent of grafted soft tissue on avascular root surfaces, whereas secondary root coverage is due to creeping attachment as described by Goldman [10]. This creeping attachment is a postsurgical migration of the gingival margin in an upward direction, to cover partially or completely previously exposed root surface.
FGG produces significant results and improvements in the recession depth, probing depth, CAL and width of keratinized gingiva. The surgical outcome highly depends on the case selection based on the patient-related and tooth/site-related factors, technical factors, and operator’s skill and experience [11].
Summary
Successful and predictable root coverage has been reported using free gingival autografts. Despite the fact that other effective root coverage techniques have been developed, the free gingival graft is still the treatment of choice for gingival recession, speciallly when an increase in the apicocoronal dimension of the keratinized gingival tissues is a desirable treatment outcome in cases with shallow vestibular depth and cases with inadequate gingival tissue where restorations with subgingival margins are to be placed.
References
- Kassab MM, Cohen RE (2003) The aetiology and prevalence of gingival recession. J Am Dent Assoc 134: 220-225.
- Björn H (1963) Free transplantation of gingiva propria. Sveriges Tandlak T.
- Nabers JM (1966) Free gingival grafts. Periodontics 4: 243- 245.
- Amler MH, Johnson PL, Saman I (1960) Histological and histochemical investigation of human alveolar socket healing in undisturbed extraction wounds 61: 32-44.
- Baer PN, Benjamin SD (1981) Gingival grafts: A historical note. J Periodontol 52: 206-207.
- Borghetti A, Gardella JP (1990) Thick gingival autograft for the coverage of gingival recession: A clinical evaluation. Int J Periodontics Restorative Dent 10: 216-229.
- Miller PD Jr (1985) Root coverage using the free soft tissue autograft following citric acid application. III. A successful and predictable procedure in areas of deep-wide recession. Int J Periodontics Restorative Dent 5: 15-37.
- Bernimoulin JP, Luscher B, Muhlemann HR (1975) Coronally repositioned periodontal flap. Clinical evaluation after one year. J Clin Periodontol 2: 1-13.
- Nobuto T, Imai H, Yamaoka A (1988) Microvascularization of the free gingival autograft. J Periodontol 59: 639-646.
- Sullivan HC, Atkins JH (1968) Free autogenous gingival grafts. Utilization of grafts in the treatment of gingival recession. Periodontics6: 152-160.
- Camargo PM, Melnick PR, Kenney EB (2000) The use of free gingival grafts for aesthetic purposes. Periodontology 27: 72-96.
Citation: Vijay S, ChatterjeeD, Meena R, KapoorA (2021) Surgical Management of Gingival Recession Using free Gingival Autograft: Case Series. J Dent Oral Health Cosmesis 6: 017.
Copyright: © 2021 Sharmistha Vijay, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.