A Case of Foster Kennedy Syndrome in a Pregnant Lady Presenting with Unilateral Deterioration of Vision
*Corresponding Author(s):
Farooq Ul AbidinResident Ophthalmology, AFIO, Rawalpindi, Pakistan
Email:fulabidin@gmail.com
Abstract
Foster Kennedy syndrome is a rare neurological entity that includes ipsilateral optic atrophy, contralateral papilledema, and sometimes anosmia. The syndrome has been described in association with a variety of intracranial pathologies such as a large frontal lobe tumor, olfactory groove meningioma, or medial third sphenoidal wing meningioma. In this report, we present a case of sphenoidal wing meningioma with Foster Kennedy syndrome in a 25-year-old pregnant female.
INTRODUCTION
Foster Kennedy in 1911 was the first to correlate the signs of unilateral optic atrophy and contralateral papilledema to space-occupying lesions in the anterior cranial fossa and emphasize its importance in localizing the masses. Although the exact localization of the lesion must be aided by detailed clinical history and other ophthalmic and neurological signs. Foster Kennedy syndrome when present hints at a visual pathway disorder and prompts further workup, including radiological imaging and neurological consultation.
CASE REPORT
A 25-year-old, 6 months pregnant female, presented to the Rehman Medical Institute Eye OPD, Peshawar, complaining of visual failure. The vision in her left eye has been declining slowly for the last 4 months but over the last week before presentation, it had fallen precipitously to counting fingers. The vision in her right eye has also deteriorated over the preceding week together with frontal headaches but not associated with nausea and vomiting. On examination, she was generally well, afebrile, alert, and oriented. Visual acuities were 6/18 in her right eye and counting fingers in the left eye not improving with pinhole or refraction. On slit lamp, anterior segment examination of both eyes was unremarkable and fundal examination revealed marked papilloedema on the right eye and optic atrophy on the left eye (Figure 1A,1B). There was no relative afferent pupillary defect, no proptosis, no bruit, and extraocular movements of both the eyes were full range. There were no other focal or generalized neurological signs.
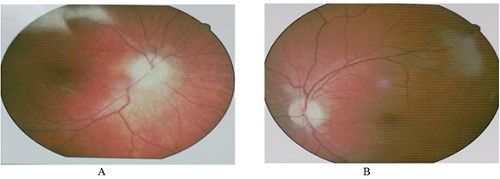 Figure 1: Optic discs at presentation showing A) Right papilloedema B) Left optic atrophy.
Figure 1: Optic discs at presentation showing A) Right papilloedema B) Left optic atrophy.
Magnetic Resonance Imaging (MRI) scan revealed an irregular large (7.3x6.6x6.6 cm) lobulated space-occupying lesion with a broad base along with the left wings of the sphenoid. The lesion shows marked suprasellar and sellar extension leading to mass effects upon optic chiasma, ipsilateral cavernous sinus, and significant contralateral midline shift (Figure 2).
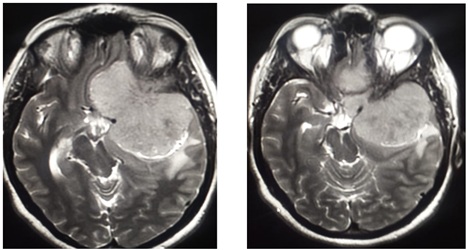 Figure 2: MRI scan at presentation showing the extent of tumor.
Figure 2: MRI scan at presentation showing the extent of tumor.
The patient was referred to the Neurology, Neurosurgery, and Gynecology department for further management.
DISCUSSION
The syndrome described by Foster Kennedy in 1911, is characterized by ‘the occurrence of true retrobulbar optic neuritis with the formation of central scotoma and primary optic atrophy on the side of the lesion together with concomitant papilloedema in the opposite eye [1]. It is most commonly associated with frontal lobe tumors, olfactory gliomas, sphenoidal meningioma. Amongst the non-tumor causes, optochiasmal arachnoiditis, sclerosis of the internal carotid artery, syphilitic basal meningitis and Paget's disease of the skull, craniostenosis, tubercular meningitis, frontal lobe abscess have been reported [2].
The pathogenesis of optic atrophy and contralateral papilloedema cannot be attributed to a single mechanism. The hypotheses include optic nerve compression causing optic atrophy together with raised intracranial pressure causing contralateral papilledema; however bilateral optic nerve compression has also been postulated [3]. The most common differential diagnosis includes the anterior ischemic optic neuropathy that sometimes shows a similar fundus picture.
Foster Kennedy syndrome is a rare entity. Tonnis found only 28 cases in a series of 3033 intracranial tumors [4]. This represents an overall incidence of less than 1%. Meningioma accounts for 15% of all intracranial tumors [5]. Risk factors for the development of meningiomas include chromosome deletion, previous ionizing therapy, and head trauma [6]. Meningiomas may progress following contraceptive implants, during the luteal phase of the menstrual cycle, or during pregnancy [7].
Symptoms include Visual loss in 70% of cases, visual field defects, usually a central scotoma, in 9%, and extraocular motility limitation in 6% [8]. Headache and anosmia are also often present. Other common complications depend on the area of intracranial involvement and potentially include nausea, vomiting, vertigo, hearing loss, memory loss, limb weakness, and facial paresis.
Management of meningiomas during pregnancy is challenging and often requires a multidisciplinary approach. The decision for surgical excision of the tumor before delivery depends on the mother’s neurological condition, the tumor histological type as well as the gestational age [9]. CT scan carries the risk of ionizing radiation to the fetus but can be considered in selected cases given its low-cost easy availability [10].
CONCLUSION
In conclusion, this was a rare and challenging case of true Foster Kennedy syndrome secondary to sphenoidale meningioma presenting in a young pregnant female.
REFERENCES
- Kennedy F (1911) Retrobulbar neuritis as an exact diagnostic sign of certain tumors and abscesses in the frontal lobes. The American Journal of the Medical Sciences 142: 355-368.
- Schatz NJ, Smith JL (1967) Non-tumor causes of the Foster Kennedy syndrome. J Neurosurg 27: 37-44.
- Watnick RL, Trobe JD (1989) Bilateral optic nerve compression as a mechanism for the Foster Kennedy syndrome. Ophthalmology 96: 1793-1798.
- Tönnis W (1962) Diagnostik der intrakraniellen Geschwülste. Klinik und Behandlung der Raumbeengenden Intrakraniellen Prozesse III, Springer, p. 1-579.
- Nanda A, Vannemreddy P (2008) Recurrence and outcome in skull base meningiomas: do they differ from other intracranial meningiomas? Skull Base 18: 243-
- Nakamura M, Struck M, Roser F, Vorkapic P, Samii M (2007) Olfactory groove meningiomas: clinical outcome and recurrence rates after tumor removal through the frontolateral and bifrontal approach. Neurosurgery 60: 844-52.
- Cowppli-Bony A, Bouvier G, Rué M, Loiseau H, Vital A, et al. (2011) Brain tumors and hormonal factors: review of the epidemiological literature. Cancer Causes Control 22: 697-714.
- Sendrowski D, Bronstein M, Lingua R (2005) Pseudo-Foster Kennedy syndrome secondary to malignant hypertension. Clinical and Refractive Optometry 16: 6-14.
- Lynch JC, Gouvêa F, Emmerich JC, Kokinovrachos G, Pereira C, et al. (2011) Management strategy for brain tumour diagnosed during pregnancy. Br J Neurosurg 25: 225-230.
- Bonfield CM, Engh JA (2012) Pregnancy and brain tumors. Neurologic clinics 30: 937-946.
Citation: Mehmood A, Abidin FU, Khan S (2021) A Case of Foster Kennedy Syndrome in a Pregnant Lady Presenting with Unilateral Deterioration of Vision. J Ophthalmic Clin Res 8: 076.
Copyright: © 2021 Asif Mehmood, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.