Journal of Ophthalmology & Clinical Research Category: Clinical
Type: Research Article
A Tricky Case of Refractive Disorder in a Female Teenager
*Corresponding Author(s):
Georgios D PanosDepartment Of Ophthalmology, Geneva University Hospitals, Alcide- Jentzer 22, CH 1211, Geneva, Switzerland
Tel:+41 767459028,
Fax:+41 223828382
Email:gdpanos@gmail.com
Received Date: Nov 25, 2014
Accepted Date: Apr 13, 2015
Published Date: Apr 27, 2015
Abstract
We present a tricky case of a teenage female patient who has been initially misdiagnosed as a case of optic neuropathy. A detailed examination including cycloplegic refraction revealed that the patient presented accommodative disorders because of latent hyperopia and previous stressful situation.
Every young patient coming in Ophthalmology service complaining for blurred vision, regardless of his age, or ocular past, need to have a cycloplegic objective refraction.a
Every young patient coming in Ophthalmology service complaining for blurred vision, regardless of his age, or ocular past, need to have a cycloplegic objective refraction.a
Keywords
Accommodative disorders, Cycloplegia, Optic neuropathy, Refractive errors
INTRODUCTION
Refractive disorders are a common condition found in the children. Fulton et al., [1] described a rate of 19% astigmatism of normal infants, at least twice the incidence in adults. Female sex, higher grade level and using computers regularly were significantly associated with refractive error according to Sewunet et al., [2]
For undiagnosed patients, who compensated during childhood, it can be made manifest in an acute way during adolescence. Accuracy of accommodation is reduced in uncorrected children with high astigmatism and high hyperopia [3]. Then the complaints can be very large and it becomes tricky for the clinician to make the diagnosis.
For undiagnosed patients, who compensated during childhood, it can be made manifest in an acute way during adolescence. Accuracy of accommodation is reduced in uncorrected children with high astigmatism and high hyperopia [3]. Then the complaints can be very large and it becomes tricky for the clinician to make the diagnosis.
CASE REPORT
In our center, a 14-year-old girl described decrease of visual acuity in the right eye since 3 weeks, without any pain or redness. She did a major depressive disorder leading to hospitalization 2 months before, and was under citalopram for a short period. Except that, she had no other past medical or ocular history.
On examination, best-corrected visual acuity was 0.3 decimal Snellen units in the right eye (+0.25/0/0) and 0.8 decimal Snellen units in the left eye (+0.25/+0.25/65). Pupils were isocore, normoreactive, with no relative afferent pupillary defect. Anterior segment examination was unremarkable in both eyes. Fundus examination was also normal, without any optic nerve abnormality.
The Lang stereo test II score was 2/4 (200moa). The Hardy-Rand-Rittler color vision test score was 21/24 in the right eye, 24/24 in the left eye.
Visual field (Octopus System) revealed numerous peripheral absolute defects in every quadrant of the right eye (Figure 1), with a relative good respect of the macular area; no defect was found in the left eye. Answers of visual evoked potentials were normal and symmetrical, for monocular and binocular vision. An optical coherence tomography (Heidelberg Engineering) was also normal both eyes.
On examination, best-corrected visual acuity was 0.3 decimal Snellen units in the right eye (+0.25/0/0) and 0.8 decimal Snellen units in the left eye (+0.25/+0.25/65). Pupils were isocore, normoreactive, with no relative afferent pupillary defect. Anterior segment examination was unremarkable in both eyes. Fundus examination was also normal, without any optic nerve abnormality.
The Lang stereo test II score was 2/4 (200moa). The Hardy-Rand-Rittler color vision test score was 21/24 in the right eye, 24/24 in the left eye.
Visual field (Octopus System) revealed numerous peripheral absolute defects in every quadrant of the right eye (Figure 1), with a relative good respect of the macular area; no defect was found in the left eye. Answers of visual evoked potentials were normal and symmetrical, for monocular and binocular vision. An optical coherence tomography (Heidelberg Engineering) was also normal both eyes.
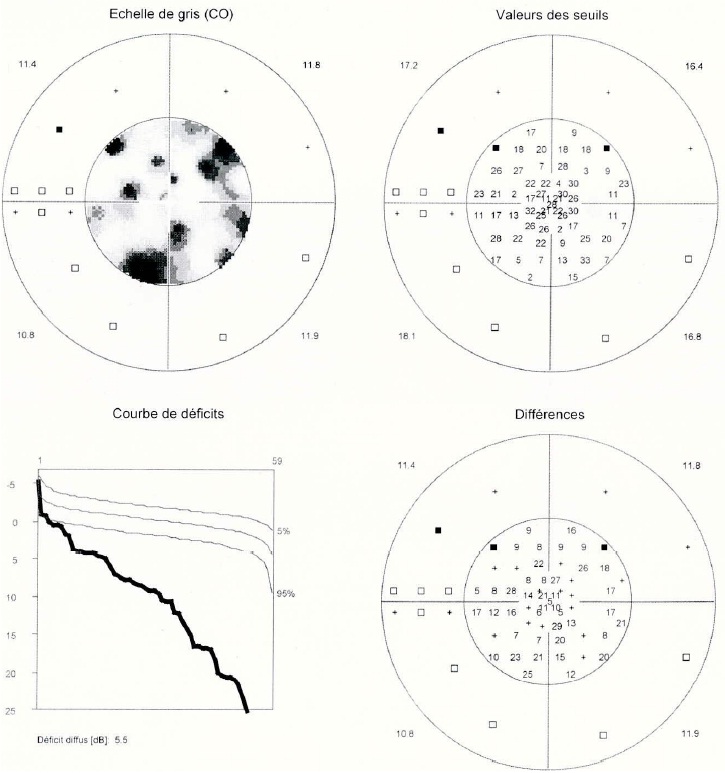
Figure 1: The first visual field examination revealed numerous peripheral absolute defects in every quadrant of the right eye.
Considering the possible diagnosis of right optic nerve lesion, like retrobulbar neuritis, brain tumour, or multiple sclerosis, we organized an urgent cerebral and orbit MRI with contrast product Gadolinium. It didn’t show any abnormality at last.
Ten days later, we found a better best-corrected visual acuity at 0.8 decimal Snellen units both eyes, with a different refraction (OD -1), and Lang stereotest I was 3/3 (1200 moa). The rest of the examination was without any particularity. These last results tend to conclude to a refractive and accommodative disorder.
Consequently, we organized a cycloplegia, according to the protocol following: one drop of oxybuprocaïne, and then three drops of cyclopentolate 0.5% every 10 minutes. After that, we did an objective refraction with autorefractometer (Retinomax) and manual skiascopy.
The visual acuity with the correction of cycloplegic refraction was 1.0 decimal Snellen units in both eyes (OD +1/+0.5/70, OS +1.5/+0.25/65). Five days later the visual field examination and visual evoked potentials were within normal limits (Figure 2).

Figure 2: Five days later, the visual field examination was within normal limits.
Finally diagnosis was hypermetropia, astigmatism, and accomodative disorders. So the problem was resolved by a prescription of adapted glasses (OD +0.50/+0.50/70, OS 0.75/+0.25/65).
DISCUSSION
Refractive disorders can cause many complaints, overall on a teenager. Visual field defects or color vision abnormalities with poor visual acuity can be misdiagnosed like optic neuritis [4].
Fulton and al [1] explained that more than one-half of astigmatic infants were screened only with cycloplegia. Even if atropine is the gold standard, the cyclopentolate-tropicamide combination is satisfactory for routine cycloplegia in children [5,6]. Atropine causes indeed prolonged blurred vision contrary to the cyclopentolate, and could potentially have a disastrous effect on the development of vision in the youngest patients [7].
To take the most possible adapted refractive measures, there are a lot of machines. Here we use Retinomax, known for diagnosing abnormal astigmatism (> or = 2 D) with 51% to 84% sensitivity rates and 98% to 90% specificity rates, depending on the chosen threshold of manifest astigmatism [8]. Moreover, this tool does easy feasible measurements in very young children thanks to quick mode, with no significant difference between the quick one and the normal one in measuring manifest refraction.
Fulton and al [1] explained that more than one-half of astigmatic infants were screened only with cycloplegia. Even if atropine is the gold standard, the cyclopentolate-tropicamide combination is satisfactory for routine cycloplegia in children [5,6]. Atropine causes indeed prolonged blurred vision contrary to the cyclopentolate, and could potentially have a disastrous effect on the development of vision in the youngest patients [7].
To take the most possible adapted refractive measures, there are a lot of machines. Here we use Retinomax, known for diagnosing abnormal astigmatism (> or = 2 D) with 51% to 84% sensitivity rates and 98% to 90% specificity rates, depending on the chosen threshold of manifest astigmatism [8]. Moreover, this tool does easy feasible measurements in very young children thanks to quick mode, with no significant difference between the quick one and the normal one in measuring manifest refraction.
CONCLUSION
To conclude, every young patient coming in Ophthalmology service complaining for blurred vision, regardless of his age, or ocular past, need to have a cycloplegic objective refraction. Refractive disorders are indeed potentially discomfortable for the patient, misdiagnosed by the Ophthalmologist, whereas they are easy to detect and treat.
REFERENCES
- Fulton AB, Dobson V, Salem D, Mar C, Petersen RA, et al. (1980) Cycloplegic refractions in infants and young children. Am J Ophthalmol 90: 239-247.
- Sewunet SA, Aredo KK, Gedefew M (2014) Uncorrected refractive error and associated factors among primary school children in Debre Markos District, Northwest Ethiopia. BMC Ophthalmol 14: 95.
- Harvey EM, Miller JM, Apple HP, Parashar P, Twelker JD, et al. (2014) Accommodation in astigmatic children during visual task performance. Invest Ophthalmol Vis Sci 55: 5420-5430.
- Pérez-Cambrodí RJ, Gómez-Hurtado Cubillana A, Merino-Suárez ML, Piñero-Llorens DP, Laria-Ochaita C (2014) Optic neuritis in pediatric population: a review in current tendencies of diagnosis and management. J Optom 7: 125-130.
- Celebi S, Aykan U (1999) The comparison of cyclopentolate and atropine in patients with refractive accommodative esotropia by means of retinoscopy, autorefractometry and biometric lens thickness. Acta Ophthalmol Scand 77: 426-429.
- Alimgil ML, Erda N (1992) The cycloplegic effect of atropine in comparison with the cyclopentolate-tropicamide-phenylephrine combination. Klin Monbl Augenheilkd 201: 9-11.
- Ingram RM, Barr A (1979) Refraction of 1-year-old children after cycloplegia with 1% cyclopentolate: comparison with findings after atropinisation. Br J Ophthalmol 63: 348-352.
- Cordonnier M, Dramaix M (1999) Screening for refractive errors in children: accuracy of the hand held refractor Retinomax to screen for astigmatism. Br J Ophthalmol 83: 157-61.
Citation: Roquelaure D, Panos GD (2015) Self-Inserted Rectal Foreign Bodies, Still a Challenging Diagnosis. J Ophthalmic Clin Res 2: 010.
Copyright: © 2015 Daniel Roquelaure, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
© 2026, Copyrights Herald Scholarly Open Access. All Rights Reserved!