Abnormal Insertion of the Inferior Oblique Muscle: A Report of 2 Cases
*Corresponding Author(s):
Dohvoma VADepartment Of Ophthalmology And Ent, Faculty Of Medicine And Biomedical Sciences, University Of Yaoundé I, Cameroon
Email:andinv@gmail.com
Abstract
Abnormal insertion of the inferior oblique muscle is rare. The authors report 2 cases observed during surgery for primary comitant exotropia. The patients presented no associated vertical deviation nor head tilt preoperatively. There was no under action or overaction of any muscle including the inferior oblique on motility testing. The inferior oblique muscle was repositioned to its normal anatomic position. Great care should be taken during lateral rectus muscle surgery to identify the inferior oblique muscle.
INTRODUCTION
Congenital abnormal insertions of extraocular muscles are not uncommon. They might be isolated or associated to craniofacial syndromes [1]. There are a few reports of isolated abnormal insertions of the horizontal recti muscle [2-4]. Isolated abnormal insertions of the oblique muscles are uncommon. We report 2 cases of abnormal insertions of the inferior oblique muscle.
CASE 1
A 9-year old boy presented with a large angle comitant exotropia which was noticed in the first year of life. Vision was 20/20 in each eye. Anterior segment examination and fundus were normal in each eye. There was a 45 Prism Diopter (PD) exotropia (Figure 1). There was no under-action or over-action of any muscle, including the inferior oblique. The right eye was the fixating eye. Under general anesthesia, the position of the fixating eye was unchanged, while the non-fixating eye showed less divergence. Unilateral recess-resect procedure on the no-fixating eye was our carried out. A 7 mm medial rectus resection was done through a limbal incision. The lateral rectus muscle was also approached by a limbal incision. After dissection, a thick fleshy tendon was hooked (Figure 2). Full-thickness bites were passed at the edges to secure the muscle. The muscle was cut close to the insertion. An anomalous insertion of the inferior oblique muscle was noticed along an oblique line (upward and backward), just beneath the lateral rectus muscle with partial fusion to the inferior border of the lateral muscle tendon. No other belly was found upon careful examination of the inferior temporal quadrant. The inferior oblique muscle was secured and cut, to allow for the lateral rectus to be recessed. A 10mm recession of the lateral rectus was done. The inferior oblique muscle was sutured to the sclera 10 mm behind the lower border of the lateral rectus muscle tendon. Post operatively, the patient was orthotropic (Figure 3).
 Figure 1: Large angle exotropia.
Figure 1: Large angle exotropia.
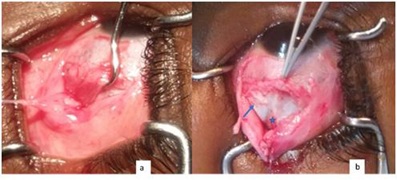 Figure 2: a) hook engaging thick fleshy tendon of the lateral rectus muscle; b) forceps holding lateral muscle tendon. Tendon (arrow) and some fibers (star) of the inferior oblique muscle.
Figure 2: a) hook engaging thick fleshy tendon of the lateral rectus muscle; b) forceps holding lateral muscle tendon. Tendon (arrow) and some fibers (star) of the inferior oblique muscle.
 Figure 3: Orthotropia following surgery.
Figure 3: Orthotropia following surgery.
CASE 2
A 30-year old male patient presented with large angle comitant exotropia since birth. Corrected vision was 20/20 in each eye. Ductions and versions were normal. The angle of deviation was 50 PD. There was mild reduction in the deviation under general anesthesia, with both eyes in abduction. In the left eye, the medial rectus was resected by 9 mm and the lateral rectus was recessed by 11 mm. The lateral rectus of the right eye was approached through a limbal incision. After dissecting, hooking and securing the muscle, it was cut close to its insertion. An anomalous insertion of the inferior oblique muscle was seen behind the tendon of the lateral rectus (Figure 4). No other belly was found upon careful examination of the inferior temporal quadrant. The inferior oblique muscle was secured and cut, to allow for the lateral rectus to be recessed. An 11mm recession of the lateral rectus was done. The inferior oblique muscle was sutured to the sclera 10 mm behind the lower border of the lateral rectus muscle tendon. Post operatively, there was 6 PD of residual exotropia, with no vertical deviation.
 Figure 4: forceps holding lateral rectus tendon and hook engaging inferior oblique muscle.
Figure 4: forceps holding lateral rectus tendon and hook engaging inferior oblique muscle.
DISCUSSION
Abnormal insertions of extraocular muscles are mostly reported by surgeons who observe these during surgery. For horizontal recti muscles, they may either mimic a palsy or a comitant strabismus [3,4]. For oblique muscles, a suspicion of an abnormal insertion could be made during clinical examination, as the case of severe superior oblique overaction in relation to an abnormal insertion of the superior oblique muscle [5]. Others might present no under-action or over-action as the case of an abnormal insertion of the inferior oblique muscle reported by Prakash et al in which the patient presented no associated `A' or `V' phenomenon, no under action or overaction of any muscle, including the inferior oblique [6].
In the case reported by Prakash et al., a fleshy mass was a part of the inferior oblique muscle, with its insertion 5 mm above the upper border of the lateral rectus. The anterior edge of the insertion was 10 mm behind the insertion of the lateral rectus muscle. In our cases, the full length of the inferior oblique muscle tendon was beneath the lateral rectus muscle, such that recession of the lateral rectus muscle along its trajectory was not possible. This is the reason why we disinserted the inferior oblique muscle and sutured it at its normal anatomic site.
The insertion of the inferior oblique is normally situated beneath the inferior border of the lateral rectus muscle, the anterior most edge being 2.2 mm underneath the lateral rectus muscle and 9 to 10mm behind the insertion of lateral rectus muscle. In the cases we report, it was directly beneath the lateral rectus muscle tendon.
CONCLUSION
Anomalous insertion of the inferior oblique muscle makes it is prone to injury while operating on the lateral rectus muscle. Strabismus surgeons should pay attention to inspect muscles per operatively.
PATIENT CONSENT
The authors certify that they have obtained consent from the adult patient and from the parent of the child to publish this manuscript. They understand that efforts will be made to conceal their identity.
CONFLICT OF INTEREST
The authors report no conflict of interest.
REFERENCES
- Wine SB, Saad N, Vella ME (2000) Bilateral inferior insertion of lateral rectus muscles associated with schizencephaly. Clin Exp Ophthalmol 28: 69-70.
- Rosenbaum AL, Jampolsky A (1975) Pseudoparalysis caused by anomalous insertion of superior rectus muscle. Arch Ophthalmol 93: 535-537.
- Okano M, Matsuo T, Konishi H, Hasebe S, Tadokoro Y, et al (1990) Anomalous posterior insertion of medial rectus muscle simulating congenital oculomotor palsy. Jpn J Ophthalmol 34: 275-279.
- Choi H, Kim H, Jeon H (2016) Abnormal medial rectus insertion presenting exotropia: a case report and review of the literature. Int J Ophthalmo l9: 1852-1854.
- Park SW, Kim HG, Heo H, Park YG (2009) Anomalous Scleral Insertion of Superior Oblique in Axenfeld-Rieger Syndrome. Korean J Ophthalmol 23: 62–64.
- Prakash P, Nayak BK, Menon V (1983) Abnormal insertion of inferior oblique. Indian J Ophthalmol 31: 21-22.
Citation: Dohvoma VA, Ebana Mvogo SR, Mvilongo TC, Chilla F, Ebana Mvogo C (2019) Abnormal Insertion of the Inferior Oblique Muscle: A Report of 2 Cases. J Ophthalmic Clin Res 6: 061.
Copyright: © 2019 Dohvoma VA, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.