Migratory Flows in the Covid-19 Era
*Corresponding Author(s):
Cruz Garcia LiriosDepartment Economy, Universidad Autonoma Del Estado De, Mexico
Email:garcialirios@uaemex.mx
Abstract
Gross mode, the relationship between migration, health and development has been undertaken through governance, as a result of an identity process that is reduced to the choice of dominant groups such as the dominated and dominated cultures such as migrants. In that sense, the differences between leaders and followers lie in: a) their access to information disseminated by the State in the media. b) Its ability to process information, ethics and logic alluding to risk and resilience. c) Legitimization of differences based on mistrust of public administration and management. In this way, the objective of this paper is to highlight the limits of the literature consulted with respect to identity, considering as a hegemonic and preponderant factor the explanation of the continuum of: migration, health and endogenous development (local or regional). To this end, a non-experimental, exploratory, cross-sectional and correlational study was carried out, with a non-probabilistic selection of 100 workers, including leaders, both migrants and natives from a central Mexican location. The results show that the intentions of occupational health determine the behaviors of the so-called self-care, but these were discussed in light of the findings reported in the literature. There are lines of research with other variables, which explain in detail the sense of community, as well as occupational health and social entrepreneurship.
Keywords
Governance; Local development; Migratory flows; Public health
Introduction
Regional development, economic and demographic sense has been understood because of public policy in which the state is assumed the guiding principle of production, employment and public services. In this scheme, the central government not only establishes a direct communication with local governments but also that, in addition, establishes a synergy with the communities or neighborhoods peripheral to the cities. In this way, the state administration is coupled with civil self when adjusting policies to the needs, expectations and local capacities [1]. This is how local policies include: i) Programs derived from universal norms, but targeted technical assistance and subsidized funds between different levels of government. ii) Operational structure, technical coordination, social linkage, citizen follow-up and community participation. iii) Technical training, information dissemination and sectorial linkage. iv) Co-investment management, transparency and corresponsability [2].
The most obvious model of regional development is known as import substitution and this sum consisted of: 1) A promoter developmental state through the most successful industrial sector. 2) Implementation of subsidies to the consolidated industry in the agro-industry. 3) Business development policies of MSMEs, as suppliers and consumers of the consolidated industry; 4) Production and transference knowledge through an educational system, as well as health and employment and 5) Infrastructure: banking, commercial, port, road, rail, electric, telecommunications and tariff [3]. However, the regional development model for import substitution stagnated national production due to protectionism and lack of competitiveness, the demand for quality in the domestic market and consumer behavior; as well as the wave of corruption among decision-makers , undermined the stabilizing project and led to inflationary and devaluation economic crises that the country could not or could not overcome [4].This is how the model of import substitution was replaced by the neoliberal model, which consists of: A) Reduction of the State's economic participation to a mere function as a gendarme. B) Suppression of public expenditure. C) Commercial and financial opening. D) Privatization of banks and companies in the State. E) Subsidy elimination or price control. F) Control of the private sector and economy. G) Free floating the national currency against the dollar. H) End of the agrarian reform, suppression of the distribution, dissolution of privatization of the field. I) reform of tax collection. J) Promotion of foreign investment [5].
It was a model adjusted to the guidelines of multilateralism dictated by international financial organizations, as well as the famous Washington Consensus, which not only accentuated the differences between developed countries and emerging economies, but also intensified increased industrial dependence, financial and technological among them [6]. In this way, the state generated a climate of confidence in direct foreign investment, as well as speculative financial capitalism, which affected the policies of health, education and employment; main axes of human development. Through the financial and commercial liberation, the deregulation of the productive sectors generated labor and occupational uncertainty that had an impact on public health in general. The commercial flexibilization and the precarization of the labor conditions reduced the occupational health of the sectors and the organizations, undermining the generation of employments and restraining so much the entrepreneurship like the creativity and the innovation [7]. Labor relations went from being solidary and cooperative to a competitive struggle for cost reduction, maximization of profits and pursuit of utility. This led to a system of formative and labor violence , which is characterized by a climate of distrustful relationships, low commitment, lack of entrepreneurship and spurious innovation; factors each and every one of them, determining the deterioration of labor relations and unhappiness [8].
Both models, both import substitution, as called neoliberal, they inhibited the participation of the productive civil sectors, they avoided the agreements and the co-responsibilities among the state, employer and worker actors [9].
While the import substitution model opted for state intervention in the economy, investment planning, strategic alliances between industrial consolidated and MSMEs; this through nationalization, regulation, promotion and subsidy, as well as the diversification of cooperative, private and community organizations, redistributing profits as if they were a national heritage. Situation that generated rather a corruption focused on nepotism and opacity, before the inflationary crises due to international trade imbalances [10], For its part, it’s the neoliberal model focused its efforts on exports as a strategy for stability and even surplus through free market, adopt a posture of gendarme, concentrating income, control inflation; This did not prevent it from acquiring fiscal deficits due to its dependence on creditors, the generation of poverty, the intensification of economic and social inequality, as well as its excessive concentration in private initiative [11]. Direct result of both models: the country has of 53.3 million poor people, of whom 36.6 million live in urban areas, while 16.7 million in rural areas. For its part, the State of Mexico, Veracruz, Puebla, Jalisco, Guanajuato and Mexico City, they have 51% of the poor [12], to scenario, the analysis of regional development seems now look to a new horizon, no longer focused on the so - called private initiative as the central players, but now, rather citizenship itself as a major player of their own development, their welfare and their own quality lifetime [13]. In other words and although it sounds stark, while governments are immersed between multilateralism and regionalism and the private initiative between the lag and the so-called: on - technological specialization, civil society, for its part, He has the unique opportunity to self-manage and self-manage his resources with and without participation in the private sector [14]. However, the first requirement for civil society to be organized around productive projects is health and education. Mainly health services are the driver of a subjective well - being and quality of life sufficient for the development of skills, abilities and knowledge hub, which come to transform local life and regional. The item of education should be left for another opportunity, without implying reducing or diminishing its importance [15].
In this vein, the landscape of public health and especially that concerning occupational, is far from favorable. The morbidity rate correlates negatively, directly as significantly as economic progress. In a limited sense, public health only consists of the proliferation of diseases that, from this perspective, would not have a direct influence on productivity, competitiveness and local economic development.However, in an intermediate perspective, public health is an ideal of a community that aspires to so-called self - care, and based on this lifestyle, subjective well-being and quality of life, limited by personal satisfactions, are expected. Finally, in a broad, broad sense of public health, she It comes to explain various processes various multidimensional inequality [16].
However, a limited vision limits the combat of origin and the consequences of public health. While a broad, vision is ambiguous and difficult to implement. Therefore, the intermediate approach allows the actors involved delimiting their opportunities and capacities to the environment, as well as to the capacities of the civil organization, among which are the health professionals [17]. Therefore, the study of the problems of public health not only possible to anticipate possible scenarios of endogenous development, but also generate alternative civil participation that contribute to health professionals in building self-management and self-administration, talents and resources of civil society that enhance the competitive advantages of their micro , small and medium enterprises; generating the employment that the intermediate sectors require to produce knowledge and transfer it to MSMEs [18], not many years ago, the State led, from its governing role , public health policies and programs; however, relatively early this paradigm changed with the emergence of migrant communities in developed countries and emerging economies being experienced by migrants to reach suburbs of cities that require them to perform jobs that natives or even Migrants from previous generations no longer want to perform [19].
In this scenario of centrality and economic migrant fair, the public’s mudslide has emerged as a central issue on the agenda of the developed and emerging countries, ejectors and receivers of migrants. Public health systems today are questioned because they care for the migrant population; vulnerable, excluded and marginal, it is in considering the public health impact of epidemics or pandemics that are born in the suburbs and end up in urban service centers [20]. Indeed, the relevance of the diagnosis of social services health public, it is essential to clarify the impact of budget cuts institutions and health centers public and their health effects in peri-urban areas [21]. Construction of a policy of public health would start from the reception and care of migrants, through health campaigns, to training of cadres according to their beliefs, perceptions and attitudes to disease; sick and professional of public s avalanche is a civil society strategy focused on health care workers to occupational health reaches or at least prevent disease and accident that undermine the production of goods and services [22]. L to public administration programs public s mudslide in their professionals has been characterized by its rift with civil society. In this way, the humid capital of hospitals and public health centers is a fundamental part of the stability of the care system and its preventive subsystems and additives to treatments and rehabilitation, but above all in the transfer of information regarding the prevention of diseases and accidents [23].Scenarios of social welfare, health public or possibly warn the emergence of institutional issues and organizational factors that impact the quality of services public health, consider fundamental contribution in the relationship established between organizational climate and quality of service observing adherence factors and the relationship between professionals of publics mudslide, patients and families [24]. Nowadays, it is not enough with a modern, automated and accessible public health system, it requires a preventive ethic that guides the quality of life and subjective well-being so that the State allocates funds to research and eradicates the discretion with which institutions are handled, as well as the impunity with which public health professionals, whether due to stress or lack of ethics, are handled in the face of the defenselessness of the civilian population [25].
A hierarchy of processes around which the system of prevention, treatment and adherence are motivated by health structures and knowledge management in which the vulnerable population, especiallychildren is its central objective, consistently explains the quality of life, subjective well-being and its effects on occupational health [26]. In this way, the objective of this study is to establish the axes and themes of a public agenda oriented towards the construction of public health governance as a local development strategy because of its impact on educational and professional training, the prevalence of capacities over the opportunities of MSMEs in the conjuncture of their strategic alliances [27]. A documentary study was carried out with a selection of sources indexed to repositories of Dialnet, Latindex and Redalyc, considering the period of publication that goes from 2010 to 2019, the inclusion of key words "development", "migration", "agenda", "Neoliberalism", "regionalism", "multilateralism", "public health", "occupational health", "entrepreneurship", "quality of life", "subjective well-being".Next, the information was processed with the Delphi technique, using matrices of content analysis, specifying a model and comparing it.
Methods
What are the axes of the trajectories of dependency relationships between the variables used in the review of the literature - values, beliefs, perceptions, motives, attitudes, knowledge, intentions and behaviors - in relation to the observations and weights in the context study?
Null
The correlations between the specified variables are adjusted to the correlations between the weighted variables.
Alternate
The relationships between the variables reported in the theory and the studies are different from the weighted observations.The study in comment was carried out in the municipality of Chalco de Covarrubias, located specifically in the east of the metropolitan area conurbated to the City of Mexico, belonging to the State of Mexico. In this sense, the demarcation interacts with other communities or populations such as: San Marcos Huixtoco, San Lucas Amanilalco, San Martin Cuatlalpan, Santa Maria Huexoculco, San Gregorio Cuatzingo, San Mateo Tzozo, San Pablo Atlazalpan, Santa Catarina Ayotzingo and San Juan Tezompa.
In the period from the year of 2019 to the year of 2021, the municipality of Chalco de Covarrubias, belonging to the federal state of l State of Mexico, is distinguished by a low level of kidnappings this in relation to cases nationwide. Unlike national cases, the fluctuation of state cases is greater and therefore supposes a risk scenario that affects regional development.
Although the variation of cases is greater in the State of Mexico with respect to the country, the cases that correspond to Mexico City represent a greater uncertainty regarding the rate of kidnappings at the national level and with respect to the State of Mexico.
In this way, the cases per 100 thousand inhabitants reveal that the State of Mexico is an entity linked to Mexico City; which has seen an increase in kidnappings as the period from 1997 to 2013 has elapsed.However, when looking at homicide cases it is possible to notice that these have intensified in the State of Mexico with respect to Mexico City and the rest of the country. In the period from 2007 to 2014, cases skyrocketed in 2011 in the case of the State of Mexico and one year later in Mexico City, while in the rest of the country it remained constant during the period in question.
In 2014, the state rate of the State of Mexico of femicides remained the same as the national rate, but in the case of the demarcation of study, it remained among the last places in the ranking, both at the federal and state level.
That is to say, although in the State of Mexico the kidnappings are inferior to the other federal entities, their variability would explain the homicides and femicides perpetrated in the demarcation of study, the rate remains stable in comparison to the other localities, but they reflect a climate of uncertainty that adds to the problem of migration and occupational health, having an impact on regional development.
It is a climate of violent relationships involving to not only rampant insecurity, but also a social deterioration that even if it remains stable compared to other districts, implies a contingency scenario.An exploratory, cross-sectional and quantitative study was carried out.A non-probabilistic sample selection was made of 345 migrants and natives, leaders and employees working in the construction industry and the finishing services sector, considering their residence and work environment, as well as their place of origin.56% of the respondents were men and the remaining 44% are women. 23% said they had finished the premium, 31% said they had completed secondary school, and the remaining 46% admitted that they only read and write. 45% mentioned a monthly family income of less than 3500 pesos (M = 2890 and SD = 12.24), 26% reported having earned between 3500 and 7000 pesos in the last month (M = 5467 and DE 141.25) and the remaining 29% reported having paid more than 7000 pesos in the previous month (M = 8213 and DE = 234.34). 57% said they live in a free union, 22% in single life and the remaining 21% are in marriage.
The Carreon Occupational Health Scale (2016) wasused, which includes 56 items related to values, beliefs, perceptions, motives, attitudes, knowledge, intentions and behaviors. Each item is answered with one of five options: 0 = not likely, 1 = very unlikely, 2 = unlikely, 3 = neither probable nor unlikely, 4 = very likely.
- Values: It refers to the principles that guide decisions and behaviors related to occupational health. This is the case of the item: " Workers who care miss an to his work go to the doctor".
- Beliefs: It refers to non-verifiable or verifiable information about occupational health. For example: "Mental illnesses will inhibit the functions of office workers".
- Perceptions: It refers to expectations regarding occupational health. "My boss will prioritize my knowledge, downplaying my well-being."
- Reasons: Refers to consistent ideas around occupational health. "I will prevent diseases to avoid extra work."
- Attitudes: Refers to evaluations related to occupational health. "Coursed auto - city or to benefit my personal health."
- Knowledge: Verifiable and verifiable information on occupational health. "I will have the right to preventive health".
- Intentions: Probabilities of carrying out an action related to occupational health. "If I needed more money, I would work overtime."
- Behaviors: Actions related to occupational health. "I will visit my doctor more frequently to prevent diseases."
Participants were surveyed in the facilities of their work centers, after having requested the corresponding permit with their bosses, arguing that a public university was conducting a preliminary study on occupational health and its effects on productivity and competitiveness of the micro, small and medium enterprises of the study location. Respondents were informed that the results of the study would be preliminary and would not be considered to modify working conditions, as well as income or rewards. They were asked to answer sincerely as the answers would be confidential and anonymous. The information was processed in the Statistical Package for Social Sciences (SPSS by its acronym in English, version 20). The Crombach's alpha was estimated in order to establish the consistency of the items in contexts and samples different from the study scenario. Validity was calculated with an exploratory factor analysis of principal axes with varimax rotation, previous estimate d e the adequacy and the sphericity with the Barttlet test and the Kayser-Meyer-Olkin parameter. We correlated the correlations with the Pearson parameter r and the regressions with the beta statistic. In each of the statistical parameters a range of -1 to +1 was considered, assuming that the values close to the unit would reveal an exceeded requirement to carry out the following analysis.
Results
The estimates for internal consistency were higher than the minimum required (alpha of 0.70) in each of the subscales of values (alpha of 0.734), perceptions (alpha of 0.793), beliefs (alpha of 0.752), reasons (alpha 0.7500), knowledge (alpha of 0,782), attitudes (alpha of 0,788), intentions (alpha of 0,783), intentions (alpha of 0,794) and behaviors (alpha of 0,791), as well as in the general scale (alpha of 0,790). Such findings mean that the instrument as a whole in its parts would have similar results in different contexts and samples if it had been tested in a sample representative of the study location. Therefore, the instrument is only reliable in the sample selected intentionally (Table 1).
|
R |
M |
S |
A |
F1 |
F2 |
F3 |
F4 |
F5 |
F6 |
F7 |
F8 |
|
|
|
Subscale of values (alpha of 0.734) |
|||||||||||
|
r1 |
The workers will be absent for going to the doctor |
3,35 |
1.01 |
0.701 |
04.03 |
|||||||
|
r2 |
The workers will have routine checks |
3,25 |
1.02 |
0,721 |
0,543 |
|||||||
|
r3 |
Bosses will request medical certificates |
3,25 |
1.02 |
0.704 |
0.412 |
|||||||
|
r4 |
Leaders will care about occupational health |
3,27 |
1.00 |
0.705 |
0.391 |
|||||||
|
|
Subscale of perceptions (alpha of 0.7 9 3) |
|||||||||||
|
r5 |
Leaders will care about occupational health |
2,36 |
1.01 |
0.7 94 |
0.302 |
|||||||
|
r6 |
Work implement sanitary measures |
2,83 |
1.21 |
0.7 67 |
0.456 |
|||||||
|
r7 |
The companions will take care of themselves |
2,20 |
1.93 |
0.7 99 |
0,396 |
|||||||
|
r8 |
Health will be a competitive advantage |
2,26 |
1.02 |
0.7 88 |
0,493 |
|||||||
|
|
Belief subscale (alpha of 0.752) |
|||||||||||
|
r9 |
Labor demands will be rewarded |
2.91 |
1.25 |
0,741 |
0.301 |
|||||||
|
r10 |
A promotion will allow healthy styles |
2.35 |
1.24 |
0.702 |
0.392 |
|||||||
|
r11 |
Heads ascents will be healthy |
2.32 |
1.26 |
0.743 |
0.302 |
|||||||
|
r12 |
Prevention prevents accidents and diseases |
2.10 |
1.01 |
0.750 |
0.303 |
|||||||
|
|
Subscale of motives (alpha of 0 , 756) |
|||||||||||
|
r13 |
I went to medical checkups to miss work |
2.32 |
1.06 |
0,721 |
0.401 |
|||||||
|
r14 |
Promoting the car - caring for myself |
3.04 |
1.02 |
0.723 |
0,582 |
|||||||
|
r15 |
I will use self - care to reduce risks |
3.16 |
1.01 |
0,744 |
0.405 |
|||||||
|
r16 |
Promoting healthy by m i styles. |
3.92 |
1.00 |
0,711 |
0,491 |
|||||||
|
|
Knowledge subscale (alpha of 0 , 782) |
|||||||||||
|
r17 |
I will be entitled to a salary insurance |
3.25 |
1.05 |
0,772 |
0,493 |
|||||||
|
r18 |
I will have the right to rest at work |
3.25 |
1,11 |
0,721 |
0,493 |
|||||||
|
r19 |
I will have the right to miss by medical consultation |
3.84 |
1,13 |
0.736 |
0.504 |
|||||||
|
r20 |
I will have the right to promote occupational health |
3.26 |
1,14 |
0,780 |
0.302 |
|||||||
|
|
Attitude subscale (alpha of 0.783) |
|||||||||||
|
r21 |
I will consult information to avoid accidents |
2.37 |
1.05 |
0,735 |
0.306 |
|||||||
|
r22 |
I will inquire about occupational risks |
2.34 |
1.02 |
0.761 |
0.384 |
|||||||
|
r23 |
I will go to the doctor to avoid diseases |
2.16 |
1.04 |
0,721 |
0.381 |
|||||||
|
r24 |
I medic are to work more |
2.93 |
1.05 |
0.742 |
0.301 |
|||||||
|
|
Intensity subscale (alpha of 0.794 ) |
|||||||||||
|
r25 |
If they will reward me, I would arrive early |
3.35 |
1,13 |
0.705 |
0.401 |
|||||||
|
r26 |
If you will support me, I would work at home |
3.02 |
1,15 |
0.705 |
0,493 |
|||||||
|
r27 |
If they will guarantee me a place, I would be trained |
3.36 |
1,15 |
0.756 |
0.502 |
|||||||
|
r28 |
If they recognized my worth, I would take courses |
3.26 |
1.26 |
0,714 |
0.306 |
|||||||
|
|
Behavior subscale (alpha of 0.791 ) |
|||||||||||
|
r29 |
I will reduce the consumption of sugar |
3.04 |
1.06 |
0,771 |
0.384 |
|||||||
|
r30 |
I will limit the intake of alcohol |
3.05 |
1.03 |
0.736 |
0.394 |
|||||||
|
r31 |
I will reduce the soft drinks |
3.06 |
1.05 |
0.782 |
0.401 |
|||||||
|
r32 |
I will share my lunch |
3.02 |
1.05 |
0.83 |
0.406 |
Table 1: Psychometric properties of the instrument.
Source: Prepared with study data; R = Reactive, M = Mean, S = Standard Deviation, A = Crombach's alpha, quoting the item's correlation, Extraction method: main axes, rotation: Promax. Sphericity and adequacy [χ2 =201.01 (24gl) p = 0.000: KMO = 0.671]. F1 = Values (alpha of 0.734 and 20% of the total variance explained),F2 = Perceptions (alpha of 0.793 and 17% of the variance) total explained), F3 = Beliefs (alpha of 0.752 and 15%of the total variance explained), F4 = Reasons (alpha of 0.756 and 13% of the total variance explained), F5 =Knowledge (alpha of 0.782 and 11% of the total variance explained), F6 = Attitudes (alpha of 0.783 and 9% of the total variance explained), F7 = Intentions (alpha of 0.794 and 5% of the total variance explained), F8 =Behaviors (alpha of 0.791 and 3% of the total variance explained). All items include five response options: 0 =not likely, 1 = very unlikely, 2 = unlikely, 3 = neither probable nor unlikely, 4 = very likely.
Regarding validity , understood as the correlations between indicators and established factors in order to establish dimensions of a continuum of choice, deliberation, planning, systematization and improvisation related to occupational health and with respect to local development, it is possible to warn eight factors, among which are the values that explained the highest percentage of total variance (20%), followed by the perceptions factor (17%) and the belief factor (15%), even though each of them the factors reached factorial weights above the minimum required (0.300).
Once the reliability and validity of the instrument was established, its factors were correlated to investigate the trajectories of dependency relationships. The anklebone No.2 shows significant correlations less than 0.0001 in the case of values motif (0.48), significant relationships between less than 0.001 perceptions and knowledge (0.41) and less than 0.01 meaningful relationships between beliefs with reasons, knowledge and attitudes (0.52, 0.53, 0.56 respectively), between reasons with attitudes and behaviors (0.31, 0.17 respectively), knowledge with attitudes and behaviors ( 0.30, 0, 10 respectively), between attitudes with intentions (0.28) and intentions with behaviors (0.19) (Table 2).
|
|
F1 |
F2 |
F3 |
F4 |
F5 |
F6 |
F7 |
F8 |
F1 |
F2 |
F3 |
F4 |
F5 |
F6 |
F7 |
F8 |
|
F1 |
1.00 |
|
|
|
|
|
|
|
1,657 |
0,549 |
0,549 |
0,672 |
0,490 |
0,547 |
0,540 |
0,650 |
|
F2 |
0.03 |
1.00 |
|
|
|
|
|
|
|
1893 |
0,671 |
0,498 |
0,435 |
0,532 |
0,547 |
0,603 |
|
F3 |
0.06 |
0.08 |
1.00 |
|
|
|
|
|
|
|
1,723 |
0,671 |
0,513 |
0,409 |
0,630 |
0,570 |
|
F4 |
0.48 *** |
0.04 |
0,52 * |
1.00 |
|
|
|
|
|
|
|
1,547 |
0,672 |
0,657 |
0,641 |
0,650 |
|
F5 |
0.01 |
0.41 ** |
0.53 * |
0.04 |
1.00 |
|
|
|
|
|
|
|
1,871 |
0,409 |
0,548 |
0,613 |
|
F6 |
0.03 |
0.01 |
0.56 * |
0.31 * |
0.30 * |
1.00 |
|
|
|
|
|
|
|
1,836 |
0,532 |
0,403 |
|
F7 |
0.07 |
0.06 |
0.03 |
0.01 |
0.03 |
0.28 * |
1.00 |
|
|
|
|
|
|
|
1,923 |
0,549 |
|
F8 |
0.01 |
0.08 |
0.06 |
0.17 * |
0.10 * |
O, 03 |
0.19 * |
1.00 |
|
|
|
|
|
|
|
1,804 |
Table 2: Correlations between the factors.
Source: Prepared with the study data; F1 = Values, F2 = Perceptions, F3 = Beliefs, F4 = Reasons, F5 = Knowledge, F6 = Attitudes, F7 = Intentions), F8 = Behaviors: *** < 0.0001; ** < 0.001; * < 0.01.
The correlations allowed carrying out the estimation of the trajectory analysis between the established factors, following their correlations the modeling of their relationships was carried out. Axes are values to behaviors, beliefs and behaviors towards perceptions to behavior, each one of the mid paths by factors such as motives, attitudes, knowledge and intentions.
However, only in the case of the trajectory that goes from beliefs to behaviors and that is mediated by attitudes and intentions, the indirect effect (0.19) is greater than in the other two axes (017: 0.10 respectively) . In this way, the direct determining factor is the intention (0.19), but the indirect factor is the beliefs (0.030) effect that was obtained by multiplying the incidence of beliefs on the attitudes (0.56) of these on the intentions (0.28) and the latter on the behaviors (0.19).
That is, beliefs as unverifiable information about occupational health seem to indirectly determine the behaviors of accident and disease prevention. This is so because the information disseminated by the State in the media is increasingly less credible by citizens and , therefore, this civil society carries out actions that will most likely be systematized as they are tested, determining their self - care , prevention and immediate attention of illnesses and accidents in comparison to the other axes (values and perceptions to behaviors). In other words, the values of an organization may be different or similar to those of native or migrant workers, but they will not affect healthy lifestyles. In the same tenor, the perceptions can be of risks and insecurity, not affecting self - care or prevention.
It is only in the case of beliefs that the information disseminated in the media about occupational health as the worker's responsibility seems to have a minimal effect on behaviors (Figure 1).
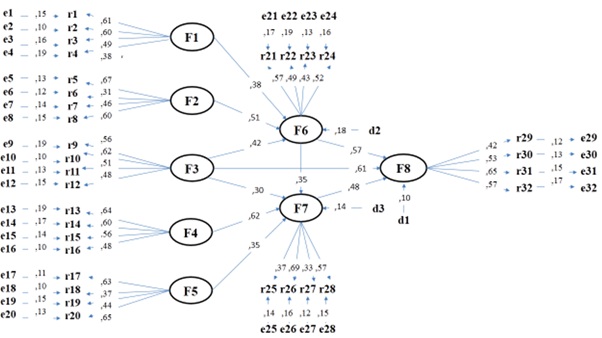 Figure 1: Structural Equation Modelling.
Figure 1: Structural Equation Modelling.
Source: Elaborated with data study; F1 = Values, F2 = Perceptions, F3 = Beliefs, F4 = Reasons, F5 = Knowledge, F6 = Attitudes, F7 = Intentions), F8 = Behaviors.
The adjustment and residual parameters [χ2 = 23, 24 (12df) p >, 05; CFI=997; GFI= 990; RMSEA=008] suggest the non-rejection of the null hypothesis relative to the significant differences between the theoretical relationships with respect to the structural model found.
Conclusion
The contribution of this work to the state of knowledge lies in establishing the reliability and validity of an instrument, which was proven in a selected sample intentionally to show the asymmetries between migrant cultures and the native, that with regard to health labor and its possible repercussions on local development. However, the present work was carried out from an exploratory study with a non-probabilistic sample selection, limiting the generalization of the results to other samples and contexts different from the one selected intentionally.
It is necessary to carry out a probabilistic and stratified sample with migrant workers and natives who work in local organizations and who are mostly immersed in the propaganda of the rectory of the State as manager and administrator of endogenous development. In this sense, a confirmatory study of the factorial structure and the trajectories of relationships between the established variables, will allow to generalize the results to the context or study scenario.
However, the findings allow discussing the limits of the theoretical, conceptual and empirical frameworks in order to delineate recommendations of public policies, although mainly contributions to self-management and self-management of occupational health by workers are exposed. In this way, the theory of social domination to notice that there are historical differences between workers and leaders not only in the relations of production but in the transfer of knowledge this work has shown that, if this information is processed as beliefs or ideas not verifiable of occupational health, then it will be possible to appreciate that the differences are due above all to the incidence of decisions on actions. This is true not only because of the irreconcilable differences between the actors, but because the workers distrust their leaders, but they exercise more control from that distrust.
In the case of social identity, the literature states that it is the sense of belonging and community that distinguishes the leaders of the workers. Even such asymmetries are observed between migrants and natives, but in the present study it has been shown that, values do not affect as much as beliefs. That is to say, that if there is a control between the leaders or between the native cultures with respect to migrant workers it is gestated in the information and not in the rooting or loyalty towards the organization, partners or trades. Regarding the rational choice that involves differences in information processing among leaders with respect to workers this document confirms this assumption since the information used as a means to achieve the purpose of control or manipulation would explain the differences between one and another group, although such asymmetries would not be observable between the natives and the migrants.
In that sense, human capital as a factor of rational decisions that enhance the capacities of leader’s vis-à-vis workers is at least questionable. That is to say, if the intentions determine the risk or preventive behaviors, then an influence greater than that obtained in the present work would be observed. Therefore, it is necessary to deepen the correlation between these two factors with samples from different groups.
Thus, in terms of intellectual capital, competitive advantage between one group of leaders and workers, or between migrant workers and native workers, it would not be consistent with the findings of this study since, although it is the intention the main determinant of a risk or preventive behavior, its relation is very close to zero and as a spurious relation it would suggest other studies related to the correlations between the indicators.
That is why reasoned action as a competitive advantage among the groups in question seems to be questionable in light of the findings of this paper. It is a deliberate process that has not only been not very predictive of behavior, but also involves a process that in relation to occupational health has been minimized by the state of knowledge and in the present study; the reported findings have been supported.
It is the same case of planned behavior as a process of systematic rationality that would lead to the prevention of accidents or illnesses, but in this work, the surveyed sample rather warns that such a planned process is spurious.
Precisely, it is the case of cognitive dissonance that would explain more convincingly the results obtained in the present work since, although the sample surveyed seems to corroborate the assumption that beliefs would have a minimal influence on risk behaviors or healthy styles of life, the findings also indicate that such influence is minimal and, therefore, the surveyed workers would rather be immersed in a work environment that needs them for their operative work, but that does not prevent them from illnesses or accidents.
It is for this circumstance relative to the dissonance that spontaneous processing approaches with greater relevance to the explanation of why migrants accept risky work, even when their occupational health is compromised. It is a scenario in which climates of relationships proliferate that influence the decisions and actions of the respondents when carrying out risk behaviors and avoiding preventive actions.
However, despite the absence of a rational, deliberate and planned process in the decision-making regarding the prevention of occupational health in the sample surveyed, it is possible to anticipate scenarios of socialization of risk rather than prevention, as would be the case of moral development in the sample surveyed. Although the values do not have a greater influence than the beliefs, the results would allow inferring an ethics of the risk that prevails over an ethics of care, as well as a logic of resistance on a logic of caution, minimum effort or the troll. A process would rather suggest that the surveyed sample trains its future workers from the ethics of risk and the logic of resistance as factors that determine their decisions and behaviors at risk to their occupational health.
This is so because risk behaviors seem to involve phases or stages of development in which future workers would forge the ethics of risk and the logic of resistance as a competitive advantage, as well as heritage of their migrant culture before the domination of the natives. Or the control of their labor leaders. In this way , the organizations in which the surveyed sample works are a mesosystem or development ecology , which promotes control and domination , this through the diffusion of the ethics of risk and the logic of resistance , as values of those who work there and expose their occupational health in order to guarantee reproductive health.
However, the most heated discussion would be with studies similar to the present, such as the relationship between migration, occupational health and local development is centered on the individual and the groups to which they belong. The authors argue that identity is the focus factor l explaining the relationship, and from this fact, the link to governance. In other words, an emerging process such as identity would explain a rather divergent process such as consensus and co-responsibilities, materialized in co-management and co-administration. Such an explanation would at least three drawbacks: 1) The identity, and this work has demonstrated no effect on the behavior under which are, in any case, multiple identities which citizenship assumes , as for example, audiences there to the information disseminated in the media. 2) The identity as an election of belonging to a group, would not be unforeseen or deliberate as stated by the authors cited, rather it would be diverse, heterogeneous and multiple, but in terms of the disseminated information and the processing capacity of the audiences. 3) Identity as a sense of community, rootedness or attachment to a place that contrasts with the values and norms of other contexts and that merges when interrelating with dominant native cultures is a collateral process to governance and, consequently, a barrier that would impede the negotiation, conciliation and shared responsibility between leaders and followers.
That is why the most relevant contribution of this study lies in the non-explanation of risk or precautionary behavior, based on variables that the state of knowledge has worked as determinants. More well this is a process still to be discovered in which, other variables explain in more detail the differences between the workers and their leaders, that with regard to occupational health; A factor that would have an impact on endogenous development through the construction of a governance system, not necessarily centered on the identity or choice of a group, place or social network.
References
- Bautista M (2013) Participation, a theoretical view of the structuring. In: Bautista M, Carreon J, Hernández J (eds.). The complexity of participation: Political, civic, community, social and autonomous. UAEMEX, Mexico.
- Bautista M, Sanchez M (2013) The multifaceted participation in Nezahualcóyotl. In: Bautista M, Carreon J, Hernández J (eds.). The complexity of participation: political, civic, community, social and autonomous. UAEMEX, Mexico.
- Bautista M, Cadena SM, Compagne JR, Castro AF, Ortiz FJ (2012) Fundamentals of the anti-global public agenda. In: Carreon J, Hernández J (eds.). Psychology of neoliberal globalization: Analysis of social exclusion, the digital divide and sustainable development. Diaz de Santos, Mexico.
- Bustos JM, Flores LM (2014) Environmental psychology, education and sustainability. In: Bustos JM, Flores LM (eds.). Environmental psychology, analysis of barriers and psychosocial facilities for sustainability. UNAM-FES Zaragoza, Mexico.
- Bustos JM, Quintero ML, García C (2017) Governance of local sustainability: Index of water mediation for Mexico City. Tlatemoani 24: 143-159.
- Carreon J (2016) Human development: Governance and social entrepreneurship. UNAM-ENTS, Mexico.
- Carreon C, Hernandez J, Morales ML, Rivera BL, Limon GA, et al. (2013) Attitudes and construction of public agenda. Realities 3: 91-105.
- Carreon J (2013) Discourses on labor migration, return and social reinsertion based on group identity in Xilitla, micro-region of HuastecaPotosina (Mexico). In: Cano L (eds.). Poverty and social inequality. Challenges for the reconfiguration of social policy. UNAM-ENTS, Mexico.
- Carreon J (2015) Quality of life in students of a public university of the State of Mexico. In: Cano L (eds.). Social policy and civil society: Remains to achieve equity and social justice. UNAM-ENTS, Mexico.
- Carreon J (2015) Contrast of a formative violence model. In: Cano L (eds.). The social problem in Mexico: A regional vision from Social Work. UNAM-ENTS, Mexico.
- Carreon J (2016) Human development: Governance, local development and social entrepreneurship. UNAM-ENTS, Mexico.
- Carreon J, Hernandez J (2013) Systems of sociopolitical insecurity: A perspective from the intervention of Social Work. In: Castro M, Chávez JC, Vazquez S (eds.). Epistemology and Social Work. UNAM-ENTS, Mexico.
- Carreon J, Hernandez J, Garcia C (2015) Migratory identity in the establishment of an agenda. Dialogues on Law and Politics 16: 69-87.
- sCarreon J, Hernández J, Quintero ML (2016) Specification of a local development model. In: Del Callejo D, Canal ME, Hernández G (eds.). Methodological guidelines for the study of development. Universidad Veracruzana, Mexico.
- Carreon J, Hernandez J, Bustos JM, Garcia C (2017) Business promotion policies and their effects on risk perceptions in coffee growers in Xilitla, San Luis Potosi, central Mexico. Poiesis32:33-51.
- Carreon J, Hernandez J, Morales ML, Rivera BL, Limon GA, et al. (2014) Towards the construction of a civil sphere of identity and public security. Realities 4: 23-36.
- Garcia C, Carreon J, Hernandez J, Aguilar JA, Rosas FJ (2016) Contrast of a model of quality of life in students of the Autonomous University of the State of Mexico. Management vision15: 8-43
- Garcia C, Carreon J, Hernandez J (2017) Limits of occupational health models. Study of adherence to the treatment of asthma in elderly migrant workers of the State of Mexico. Management Vision 16: 103-118.
- Garcia C, Carreon J, Hernandez J, Salinas (2016) Governance of the actors and networks of technological innovation. In: Quintero ML, Sales J, Velazquez (eds.). Innovation and technology Challenges for its practical application in companies. Porrua-UAEMEX UAP Nezahualcoyotl, Mexcio.
- Hernandez J, Carreon J, Garcia C, Aguilar JA, Lopez LR (2017) Reliability and validity of an instrument that measures attitudes towards sustainability. In: Quintero ML, Velazq EB, Sales (eds.). Approaches, strategy and trans discipline in the studies of sustainability. Porrua-UAEMEX UAP Nezahualcoyotl, Mexico.
- Limon GA, Rivera BL, Bustos JM, Juarez M, Garcia C (2017) Governance of climate change: Specification of a model of attitudes towards climate change governments. PoliticalScience 30: 1-31.
- Perez G, Juarez M, Carreon J, Bustos JM, Garcia C, et al. (2017) Governance of water sustainability. The Point on the i 6: 50-57.
- Quintero ML, Garcia C, Carreon J, Hernandez J, Bustos JM (2016) Governance of the quality of life and sustainable behaviors. Realities 6: 79-88.
- Roquenil MC, Umbral ME (2013) The diversity of participation: Citizen, political, social, community and autonomous. In: Bautista M, Carreon J, Hernandez J (eds.). The complexity of participation: Political, civic, community, social and autonomous. UAEMEX, Mexico.
- Sanchez A, Quintero ML, Sanchez R, Fierro E, Garcia C (2017) Governance of social entrepreneurship: Specification of a model for the study of local innovation. Nomads 51: 1-21.
- Sandoval FR, Carreon J, Garcia C, Valdes O (2015) Formalization of dependency relations between water and social variables for the management of sustainable local development. Kaleidoscope 2: 85-93.
- Sandoval FR, Carreon J, Garcia C, Quintero ML, Bustos JM (2017) Model of the determinants of the perception of resilience based on perceived risk and stress in relation to the governance of civil protection. Invurnus 12: 30-35.
Citation: Guarnero GE, Ruiz HDM, Sanchez AS, Lirios CG (2022) Migratory Flows in the Covid-19 Era. J Psychiatry Depression Anxiety 8: 44
Copyright: © 2022 Gregorio Elizarraraz Guarneros, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.