Retinal Detachment Indicative of Choroidal Metastasis of Pulmonary Adenocarcinoma
*Corresponding Author(s):
Y MouzariDepartment Of Ophthalmology, Military Hospital, Mohammed V University, Morocco
Tel:+212 658903998,
Email:ys.mouzari@gmail.com
Abstract
Introduction
Choroidal metastases are metastatic tumors of the posterior uvea and account for 80% of intraocular malignancies. They are often present in metastatic lung cancer, but they can be exceptionally revealer of this disease.
Observation
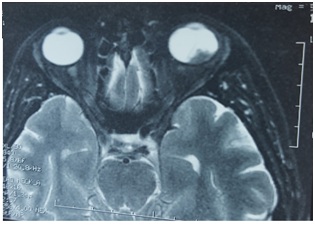
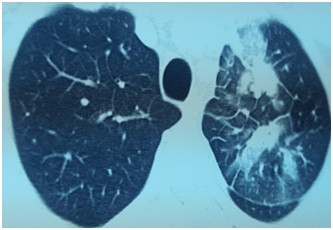
We report the case of a 38 years old man, with no particular pathological background. He was examined for a rapid visual acuity decline in the left eye. The eye fundus reveals a retinal detachment in the left eye. Orbital MRI shows a choroidal process compatible with left choroidal metastasis with retinal detachment, thoracic-abdominal-pelvic scanner reveals a pulmonary tumor process with bilateral adrenal metastases.
Discussion
Choroidal metastases are rarely revealer of lung cancer; in fact they are often present at advanced stage of the disease.
Keywords
INTRODUCTION
OBSERVATION
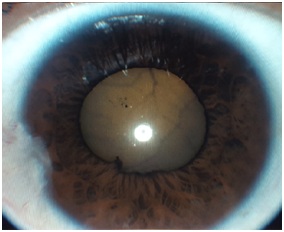
Figure 1: The picture of the anterior segment of the left eye indicates that the retina is visible in the anterior vitreous.
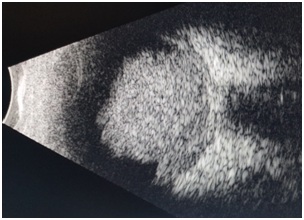
Figure 2: The B-mode ultrasound of the left eye shows an hypoechoic choroidal tumor.
DISCUSSION
CONCLUSION
CONFLICT OF INTEREST
REFERENCES
- Shields CL, Shields JA, Gross NE, Schwartz GP, Lally SE (1997) Survey of 520 eyes with uveal metastases. Ophthalmology 104: 1265-1276.
- Kreusel KM, Bornfeld N, Hosten N, Wiegel T, Foerster MH (1998) Solitary choroidal metastasis as the first sign of metastatic lung carcinoid. Arch Ophtalmol 116: 1396-1397.
- Kreusel KM, Wiegel T, Stange M, Bornfeld N, Hinkelbein W, et al. (2002) Choroidal metastasis in disseminated lung cancer : frequency and risk factors. Am J Ophthalmol 134: 445-447.
- Shields JA, Shields CS, Eagle RC Jr, Gündüz K, Lin B (1998) Diffuse ocular metastases as an initial sign of metastatic lung cancer. Ophtalmology 29: 598-601.
- Abundo RE, Orenic CJ, Anderson SF, Townsend JC (1997) Choroidal metatases resulting from carcinoma of the lung. J Am Optom Assoc 68: 95-108.
- De Potter P, Disneur D, Levcq L, Snyers B (2002) Ocular manifestations of cancer. J Fr Ophtalmol 25: 194-202.
- Wiegel T, Bottke D, Kreusel KM, Schmidt S, Bornfeld N, et al. (2002) External beam radiotherapy of choroidal metastases-final results of a prospective study of the German Cancer Society. Radiother Oncol 64: 13-18.
- Letson AD, Davidorf FH, Bruce RA Jr (1982). Chemotherapy for treatment of choroidal metastasis from breast carcinoma. Am J Ophthalmol 93: 102-106.
- Battikh MH, Ben Sayah S, Ben Sayah MM, Maatallah A, Joobeur S, et al. (2004) Choroid metastases revealing pulmonary adenocarcinoma resolved with chemotherapy. Rev Pneumol Clin 60: 353-356.
- Kaushik S, Arya SK (2003) Choroidal Metastasis from an Occult Primary. J Postgrad Med 49: 268-271.
Citation: Mouzari Y, Belfaiza S, Jeddou I , Laaribi N, Ajhoun Y, et al. (2019) Retinal Detachment Indicative of Choroidal Metastasis of Pulmonary Adenocarcinoma. J Ophthalmic Clin Res 6: 050.
Copyright: © 2019 Y Mouzari, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.